ResearchMatch
 Did you know that UConn Health is part of the ResearchMatch Network? ResearchMatch.org is a national online recruitment tool, funded by the National Institutes of Health and maintained at Vanderbilt University. ResearchMatch connects interested participants with health-related research studies that might be a good “match” for them through its secure, online matching tool. There is no cost to UConn Health researchers who use ResearchMatch to conduct recruitment feasibility analysis or participant recruitment.
Did you know that UConn Health is part of the ResearchMatch Network? ResearchMatch.org is a national online recruitment tool, funded by the National Institutes of Health and maintained at Vanderbilt University. ResearchMatch connects interested participants with health-related research studies that might be a good “match” for them through its secure, online matching tool. There is no cost to UConn Health researchers who use ResearchMatch to conduct recruitment feasibility analysis or participant recruitment.
For more information, including the process for using ResearchMatch as a recruitment tool, visit our ResearchMatch webpage or contact Ellen Ciesielski in Research Integrity & Compliance.
“Human Pluripotent Stem Cells Twenty-Five Years On” Webinar
The discovery of human pluripotent stem cells just over twenty-five years ago almost immediately engendered widespread enthusiastic speculation concerning their future potential in research and medicine: a future as models for early human development, as platforms for functional human genomics, as tools for the study of disease, drug screening and toxicology, and as a renewable source of cellular therapeutics for a range of intractable diseases. In this lecture, Dr. Martin Pera, a noted expert in the pluripotent stem cell field, will assess the progress thus far and the prospects and challenges ahead.
The UConn/UConn Health Stem Cell Research Oversight (SCRO) Committee invites you to this one-hour lecture followed by a 30-minute Q&A session!
Date: Monday, May 13, 2024
Time: 4:00 p.m. – 5:30 p.m. EDT
Presenter: Dr. Martin Pera
Topic: Human Pluripotent Stem Cells Twenty-Five Years On
Registration Link: WebEx Registration Link
Martin Pera, Ph.D., The Jackson Laboratory
Martin Pera is a Professor at the Jackson Laboratory in Bar Harbor, Maine. He is the Chair of the Steering Group of the International Stem Cell Initiative, a member of the Board of Directors of the International Society for Stem Cell Research, and Editor-in-Chief of the society’s journal, Stem Cell Reports. His laboratory when at Monash University was the second in the world to isolate embryonic stem cells from the human blastocyst, and the first to describe their differentiation into somatic cells (neurons) in vitro. His current research is focused on understanding cell state transitions in pluripotent stem cells, and on the use of pluripotent stem cells to study disorders of the central nervous system and the development of cell therapy for age-related macular degeneration. Dr. Pera’s research interests are the cell biology of pluripotency and the applications of human pluripotent stem cells in disease modeling and therapy.
For questions, contact Ellen Ciesielski, UConn/UConn Health SCRO Coordinator, Research Integrity & Compliance.
Questions about ClinicalTrials.gov?
ClinicalTrials.gov is an online database of clinical trials. At UConn Health, Principal Investigators are responsible for registering and posting results per the federal regulations as well journal policies. That National Institutes of Health definition of a clinical trial is a research study1 in which one or more human subjects2 are prospectively assigned3 to one or more interventions4 (which may include placebo or other control) to evaluate the effects of those interventions on health-related biomedical or behavioral outcomes.5
Do you have questions about ClinicalTrials.gov registration or results posting? To schedule a virtual or in-person session with the UConn Health contact for ClinicalTrials.gov, email Ellen Ciesielski, Research Compliance Monitor in Research Integrity & Compliance in the OVPR. To learn more about ClinicalTrials.gov requirements, please see our webpages.
1See Common Rule definition of research at 45 CFR 46.102(d).
2See Common Rule definition of human subject at 45 CFR 46.102(f).
3The term “prospectively assigned” refers to a pre-defined process (e.g., randomization) specified in an approved protocol that stipulates the assignment of research subjects (individually or in clusters) to one or more arms (e.g., intervention, placebo, or other control) of a clinical trial.
4An intervention is defined as a manipulation of the subject or subject’s environment for the purpose of modifying one or more health-related biomedical or behavioral processes and/or endpoints. Examples include: drugs/small molecules/compounds; biologics; devices; procedures (e.g., surgical techniques); delivery systems (e.g., telemedicine, face-to-face interviews); strategies to change health-related behavior (e.g., diet, cognitive therapy, exercise, development of new habits); treatment strategies; prevention strategies; and, diagnostic strategies.
5Health-related biomedical or behavioral outcome is defined as the pre-specified goal(s) or condition(s) that reflect the effect of one or more interventions on human subjects’ biomedical or behavioral status or quality of life. Examples include: positive or negative changes to physiological or biological parameters (e.g., improvement of lung capacity, gene expression); positive or negative changes to psychological or neurodevelopmental parameters (e.g., mood management intervention for smokers; reading comprehension and /or information retention); positive or negative changes to disease processes; positive or negative changes to health-related behaviors; and, positive or negative changes to quality of life.
HSPP-Newsletter- January-February- March, 2024
UConn Health’s HSPP Reaccreditation from the
Association for Accreditation of Human Research Protection Program (AAHRPP)
On March 27-28, 2024, UConn Health Human Subjects Protection Program (HSPP) underwent a Site Visit evaluation as part of the process of reaccreditation by the Association for Accreditation of Human Research Protection Programs (AAHRPP). After the HSPP responds to the Site Visit report the application will be reviewed by the AAHRPP Council in June 2024. This process required team work from many stakeholders. The Director of the Human Subjects Protection Program and the Associate Vice President for Research Integrity & Compliance extend their gratitude to the faculty, staff, IRB members and members of the Scientific Review and Conflicts of Interest Committees, Office of Clinical and Translational Research Services, Sponsored Program Services, Research Pharmacy and Research Safety, and many others who committed their time to the Site Visit and who ensure that we have an outstanding human subjects program every day.
FDA Regulated Research
Overview of Human Subjects Research with Devices
The U.S. Food and Drug Administration (FDA) regulates drugs, biologics, and devices used in the diagnosis, mitigation, treatment, or prevention of diseases.
Investigators who will be conducting clinical investigations in which the purpose of the study is to obtain data about a medical device (e.g., data on its safety and effectiveness), should become familiar with the information provided below to determine whether: (a) the device is exempt from an investigational device application (IDE), (b) the device fulfills the requirements for an abbreviated IDE, or (c) the device needs an IDE issued by the FDA.
Investigators should only think about these determinations when research participants of a clinical investigation will become part of the group in which a medical device will be used or part of the control group, and the device is the object of the investigation/research study.
Unless the sponsor of the device has made the determination that the device is exempt from the requirements of Part 812.2 (c), the study may be conducted under an abbreviated IDE or the investigator must submit an IDE application to FDA. See Table 1 below.
An investigational device exemption (IDE) is a regulatory status granted by the FDA that allows researchers to conduct clinical investigations on medical devices that have not yet received FDA approval. However, not all device studies are required to submit an IDE application to the FDA. If a device is determined to be a non-significant device (NSR) in concurrence with the IRB, then an IDE is not necessary.
An IRB may determine that a device is a non-significant device because it does not meet the definition for a significant risk device (SR) (see definition of SR below) and does not present a potential for serious risk to the health, safety, or welfare of participants.
The sections below explains when and how an investigator makes a determination that a device could be used in a clinical investigation under an abbreviated IDE or under an Investigational Device Exemption (IDE).
Abbreviated Investigational Device Exemption
The sponsor makes the initial determination of SR or NSR for the device. However, it is important to note the IRB will make the final determination for NSR devices. If the research study is investigator initiated, then the investigator is also acting as the sponsor.
NSR device studies may not require submission to the FDA providing they comply with the abbreviated requirements of the regulations described in the IRB Policy 2011-021.0.pdf – Investigational Device Studies
The FDA considers an investigation of a non-significant risk device to have an approved IDE (Abbreviated Investigational Device Exemption) when an IRB concurs with the initial non-significant risk determination of the sponsor or investigator and approves the study. See Table 1 below.
Investigational Device Exemption (IDE)
If either the investigator or the IRB has made a determination that the device is a significant risk device an IDE application is to be submitted to the FDA.
To obtain an IDE approval by the FDA, the sponsor or manufacturer of the device must properly fill out an IDE application. This application should be submitted proposing a human clinical researcher to study an unapproved significant risk device or a cleared or approved device for use other than its approved indication or intent.
The application should provide information about the investigational device, including its design, manufacturing process, and intended use. A clinical investigational protocol that outlines study objectives, methodology, patient population, and end points should also be included. In addition, the sponsor must demonstrate in the application that there is reason to believe that the risks to human subjects from the proposed investigation are outweighed by the anticipated benefits to subjects, the importance of the knowledge to be gained, that the investigation is scientifically sound, and that there is reason to believe that the device as proposed for use will be effective.
An IDE application can be considered approved 30 days after it has been reviewed by the FDA, unless otherwise indicated. The FDA may inform the sponsor of approval, approval with conditions, or disapproval prior to 30 calendar days from the date of receipt.
Once FDA approval is granted, and the IRB has approved the study the sponsor and/or investigator may proceed with the clinical investigation. See Table 1 below.
The FDA grants permission so a device that otherwise would be required to comply with a performance standard or to have premarket approval can be shipped lawfully for the purpose of conducting investigations of that device. This FDA permission is evidenced by the assignment of an IDE number.
Additional Points to Consider About Research Studies with Medical Devices
- Studies of SR Devices require review of the convened IRB.
- NSR device studies generally will require full board review but may be approved through the expedited review procedure if the study falls within a designated approvable category and is minimal risk.
- IRB approval must be obtained before any clinical investigation can begin, and for studies with a SR Device, both FDA and IRB approval must be obtained before any subject can be enrolled.
Definitions-
Clinical investigation means any experiment that involves a test article and one or more human subjects and that either is subject to requirements for prior submission to the Food and Drug Administration under section 505(i) or 520(g) of the act, or is not subject to requirements for prior submission to the Food and Drug Administration under these sections of the act, but the results of which are intended to be submitted later to, or held for inspection by, the Food and Drug Administration as part of an application for a research or marketing permit. The term does not include experiments that are subject to the provisions of part 58 of this chapter, regarding nonclinical laboratory studies.
Significant Risk (SR) Device: A device that presents a potential for serious risk to the health, safety, or welfare of a subject and 1) is intended as an implant, or 2) is used in supporting or sustaining human life, or 3) is of substantial importance in diagnosing, curing, mitigating or treating a disease, or otherwise prevents impairment of human health, or 4) otherwise presents a potential for serious risk to the health, safety, or welfare of a subject.
Table 1
| Categories of Research Studies with Medical Devices | |||
|
IDE Exempt |
Non-Significant Risk (NSR) |
Significant Risk (SR) |
|
| Risk | Lowest Level of Risk | Low Risk | High risk |
|
FDA Approval |
Exempt from 21 CFR Part 812 |
Must comply with an Abbreviated Investigational Device Exemption in 21 CFR Part 812.2 (b) | Must follow ALL IDE Regulations in 21 CFR Part 812-Investigational Device Exemption (IDE) Application |
| IRB Review Approval | YES | YES | YES |
Resources for investigators:
ReGARDD – Regulatory Guidance for Academic Research of Drugs and Devices
Device Advice: Comprehensive Regulatory Assistance | FDA
UConn Health IRB Forms and Polices Revisions
&
Educational Resources
The following forms have been updated:
- Instructions for Requesting Reliance Upon Advarra IRB.docx(2/13/2024, updated contacts at Advarra and consent template injury language section)
- Request for UConn Health as a Recruitment Site -Without Engagement(*new form as of 3/20/24)
The following policy has been updated:
- 2011-008.2.pdf– Informed Consent – Waivers and Alterations (1/22/2024) (including the FDA final rule that allows IRBs to approve an informed consent procedure that does not include or that alters certain informed consent elements, or to waive the requirement to obtain informed consent, for certain minimal risk clinical investigations).
The following links were added to the IRB website under online resources for investigators:
- Regulatory Guidance for Academic Research of Drug and Devices
- Is my Device Study Exempt from Investigational Device Exemption (IDE) Regulations?
Upcoming Changes in at the HSPP/IRB
Education & Development Specialist of HSPP: As of 4/5/2024, Mayra Cagganello has transferred to a new position within UConn Health. Mayra has worked for the HSPP for almost 13 years and her dedication and support to the HSPP and research community will be missed!
Investigators who need education, guidance on IRB submission and/or training with the IRIS submission system should contact the IRB at irb@uchc.edu
We wish Mayra the best in her new role!
Bibliography
2011-007.0.pdf – Definitions Applied to Policies
2011-021.0.pdf – Investigational Device Studies
March Remote RCR Training 3/26
The Responsible Conduct of Research (RCR) Office within Research Integrity & Compliance in the OVPR hosts monthly remote RCR training sessions. For our March remote event, we will be discussing several case studies. This 1-hour event will count towards the 8-hour in person requirement for NIH, however all those who conduct research are strongly encouraged to attend!
For more details about RCR requirements, please visit our RCR Program website.
For questions, please contact Research Compliance Monitor, Ellen Ciesielski or Karen Moré, Director of Research Compliance.
What: March RCR remote training session featuring case study discussions
When: Tuesday, March 26th from 12:00 p.m. to 1:00 p.m.
March RCR Training
Calling All Human Subjects Research Staff! Please join the Responsible Conduct of Research (RCR) Office for our March in-person RCR training session with a focus on clinical and social researchers!
This month, we will be highlighting the importance of appropriately protecting research participants and avoiding research misconduct. We will meet in the library to view the Office of Research Integrity’s (ORI) interactive movie: “The Research Clinic.” Snacks will be provided!
The movie is designed as a “choose your own adventure”-type experience to allow participants to work through some common pitfalls and challenges in a low-risk environment. This 1.5-hour event will count towards the 8-hour in person requirement for NIH, but we highly encourage anyone conducting human subjects research to join us!
Space is limited so registration is required. To register, please email Research Compliance Monitor, Ellen Ciesielski.
What: March RCR in-person training, “The Research Clinic”
When: Wednesday, March 13th from 12:00 p.m. to 1:30 p.m.
Where: Babbidge Library, Class of ’47 Classroom
For questions, please contact Karen Moré, Director of Research Compliance. For more details about RCR requirements, please visit our RCR Office website.
2024 Responsible Conduct of Research Training Remote Sessions
This is the last week of the 2024 Responsible Conduct of Research (RCR) training sessions! Sessions will be presented live via WebEx in a series of hour-long sessions. This week’s sessions include “Managing Mentoring and Peer Relationships” on Monday 2/26, “Research Security/Export Control” on Tuesday 2/27, “Ethics in the Use of Human Subjects in Research” on Thursday 2/29.
Who should sign up? All trainees, fellows, participants, and scholars receiving support through any NIH training grant, career development award (individual or institutional), research education grant, or dissertation research grant (specifically, the following programs: D43, D71, F05, F30, F31, F32, F33, F34, F37, F38, K01, K02, K05, K07, K08, K12, K18, K22, K23, K24, K25, K26, K30, K99/R00, KL1, KL2, R25, R36, T15, T32, T34, T35, T36, T37, T90/R90, TL1, TU2, and U2R) are required to complete RCR training per NIH policy. This policy also applies to any other NIH-funded programs supporting research training, career development, or research education that require instruction in responsible conduct of research as stated in the relevant funding opportunity announcements.
What kind of training is required? Unlike NSF or USDA NIFA RCR requirements which can be satisfied by online training through the CITI program, NIH requires training to be “face-to-face.” Specifically, 8 hours of unique face-to-face presentation material are required by NIH. The February remote RCR training sessions may be utilized to satisfy this requirement.
How do I sign up? Please visit the UConn Health RCR website for a list of the sessions offered along with registration links.
To learn more about the NIH RCR requirement or other options to satisfy NIH’s RCR training requirement, please visit the UConn Health RCR website.
Questions? Please contact Research Compliance Monitor, Ellen Ciesielski at eciesielski@uchc.edu.
OCTOBER, NOVEMBER, DECEMBER, 2023 – HSPP NEWSLETTER
OCTOBER, NOVEMBER, DECEMBER, 2023 – HSPP NEWSLETTER
The HIPAA Privacy Rule & Human Subjects Research – Overview
The HIPAA Privacy Rule (the “Privacy Rule”) may impose additional requirements to the federal human subjects protection regulations applied to all human subjects research.
The purpose of this overview is to clarify concepts and apply them to commonly seen human subjects research activities/studies. Specifically, the sections below highlight some of the main provisions of the Privacy Rule as they relate to human subjects research.
A series of questions and answers explain the scope of the Privacy Rule, the difference between an Authorization, a Waiver of HIPAA Authorization and an Alteration of HIPAA Authorization. In addition, several sections explain how to address the Privacy Rule in recruitment activities, and when using specimens for research studies. Examples of research activities and the appropriate HIPAA forms are included in some of those sections.
| Section A- Questions related to the Privacy Rule and Human Subjects Research |
The Privacy Rule regulates the way certain organizations called covered entities under the Rule handle protected health information (PHI). Since UConn Health is a covered entity, investigators conducting research with UConn Health PHI need to address HIPAA.
Question: How do I know if I need to address the Privacy Rule in my research study?
Answer: The Privacy Rule affects research and researchers when either:
Research creates or generates PHI, or research requires access to and/or use of PHI.
If your study involves the use of PHI you must address the Privacy Rule within your application for approval. PHI means individually identifiable health information transmitted or maintained in any form (electronic means, on paper, or through oral communication) that relates to the past, present or future physical or mental health or condition of an individual. Health information is not considered PHI if it has been de-identified in accordance with the Privacy Rule (i.e., by expert analysis or by removing all identifiers specified in the Privacy Rule of the individual or of relatives, employers, or household members of the individual).
Examples of research studies for which the HIPAA regulations apply are:
- Studies using individually identifiable health information that is generated as part of a health care service.
- Studies gathering individually identifiable health information that is entered into a medical record.
- Studies gathering individually identifiable health information that is used to make treatment decisions.
- Retrospective or Prospective research studies involving the review of medical records.
- Research studies involving surveys, questionnaires or focus groups, which obtain PHI from patients receiving treatment.
Question: When does the Privacy Rule not apply to research?
Answer: Research studies that do not use, disclose or create PHI are not subject to HIPAA regulations.
Examples of studies that are not subject to HIPAA:
- Studies that use tests that do not go into the medical record because they are part of a basic research study and the results will not be disclosed to the subject.
- Studies that review de-identified health information.
- Studies that obtain data from records open to the public.
- Interviews, focus groups, and surveys studies that collect information that is not considered health information (e.g., opinions, beliefs, wants/preferences, etc.)
Question: What is the difference between HIPAA “Authorization” and Informed Consent?
Answer: An informed consent is the individual’s volunteer permission to participate in the research. The requirement to obtain the legally effective informed consent of individuals before involving them in research is one of the central protections provided for under the HHS regulations at 45 CFR part 46 ( AKA as the Common Rule). The Common Rule’s focus is in protecting the safety of the individuals, their privacy, and confidentiality. To do so, the investigators need to include in the consent forms the applicable elements /information described in the Main Consent Form Checklist.doc .
The Privacy Rule, a different regulation, focuses on protecting the privacy and security of PHI. The Privacy Rule generally requires subjects to give written Authorization before a covered entity may use or disclose patients’ PHI for research. A signed HIPAA Authorization represents an individual’s agreement to the use and disclosure of the individual’s PHI for the specified research purpose.
An authorization must contain several required elements and statements, including but not limited to a description of the PHI to be used and disclosed, the person authorized to make the use or disclosure, the researcher may make the disclosure, an expiration date, and, in some cases, the purpose for which the information may be used or disclosed.
| Section B- Questions related to Waiver of HIPAA Authorization and Alteration of HIPAA Authorization |
The IRB may approve a HIPAA authorization process which does not include, or which alters some or all of the elements of a valid written authorization, or waives the requirement for written HIPAA authorization if the IRB finds and documents that the use of the subjects’ PHI meets the criteria for a waiver.
In granting an alteration or waiver of HIPAA authorization, the IRB must determine that the alteration or waiver, in whole or in part satisfies each of the following criteria:
- The use or disclosure of PHI involves no more than minimal risk to the privacy of individuals, based on, at least, the presence of the following elements:
- an adequate plan to protect the identifiers from improper use and disclosure;
- an adequate plan to destroy the identifiers at the earliest opportunity consistent with the conduct of the research, unless there is a health or research justification for retaining the identifiers or such retention is otherwise required by law; and
- adequate written assurances that the PHI will not be reused or disclosed to any other person or entity, except as required by law, for authorized oversight of the research study, or for other research for which the use or disclosure of PHI would be permitted (i.e., under the HIPAA regulations).
- The research could not practicably be conducted without the waiver or alteration; and
- The research could not practicably be conducted without access to or use of the PHI.
Question: What is the difference between a partial and complete Waiver of HIPAA Authorization?
Answer: A waiver of HIPAA authorization is a determination that is made by the IRB. An IRB can waive in full or in part the individual authorization required by the Privacy Rule to use and disclose PHI for research purposes.
Example of research study for which the IRB may grant a complete waiver of the Authorization:
- A research study limited to a retrospective review of medical records (HIPAA Waiver for the entire study).
Example of research study for which the IRB may grant a partial waiver of the Authorization:
- A research study collecting information during telephone screening (HIPAA Waiver for a portion of the study).
To request a waiver of HIPAA authorization the investigator must complete pages 1 and 2 of the HIPAA Request for Alteration or Waiver of Authorization.doc form and submit this document to the IRB for review and approval prior to using and/or disclosing PHI.
Question: Is it possible to get a HIPAA waiver to screen patient charts without having each patient first sign an Authorization form?
Answer: Yes. The Privacy Rule allows for certain activities regarding screening, recruiting or determining eligibility (e.g. chart reviews for determining eligibility) to occur without obtaining a HIPAA authorization.
The investigator must submit a HIPAA Request for Alteration or Waiver of Authorization.doc . The waiver must be granted by the IRB before charts are screened.
Question: What is a HIPAA Alteration of the Required Elements and/or Statements?
Answer: A HIPAA Alteration of the Required Elements and/or Statements is a regulatory determination that is made by the IRB. An IRB can approve to omit (waive), or change (alter) in part the individual authorization required by the Privacy Rule to use and disclose PHI for research purposes.
When investigators are planning to obtain an individual’s authorization to access their information, and they need to either remove (waive), or change (alter) some of the core elements or statements of an authorization, they must complete and submit Appendix A. Appendix A is in the fourth page of the HIPAA Request for Alteration or Waiver of Authorization.doc form The IRB must approve this request prior to the use and/or disclosure of PHI.
Example of an alteration of the authorization:
- An authorization that requires to remove (waive) the element that describes each purpose of the requested use or disclosure because providing the purpose of the study would affect the results of the study.
Examples of studies withholding information about the study purpose and/or reason for procedures, in order to prevent biasing the results:
- Subjects are asked to take a quiz for research but they are not told that the research question involves how background noise affects their ability to concentrate.
- To further understanding of how representations of same sex couples depicted in commercials influence consumer behavior, subjects are exposed to advertisements featuring gay couples and straight couples while their heart rate, facial muscle movement, and sweat responses are recorded. Subjects are informed that their reactions to the commercials are being studied, but not that the researchers are examining if the sexual orientation of characters in commercials influences them.
To request to alter the HIPAA authorization, the investigator needs to submit a HIPAA Request for Alteration or Waiver of Authorization.doc and Appendix A.
Example of research study that requires waiving documentation/signature of the authorization:
- Research on sensitive topics, such as domestic violence or illegal activities where the only link of a subject to the study is their signature on the authorization, and there is a risk of breach of confidentiality.
To request a waiver of the participant’s signature on the HIPAA authorization, the investigator needs to submit a HIPAA Request for Alteration or Waiver of Authorization.doc and Appendix A.
| Section C- Questions Related to IRB Review and the Privacy Rule when Using Specimens for Research |
Because the federal definition of human subjects research extends to people who are sources of biological specimens and identifiable private information, research with these materials often requires review and approval by the IRB. The level of IRB review is based on the level of risk the study poses.
The risks of research with specimens potentially include one or both of the following:
- The risk of harm from procedures used to obtain specimens, and/or
- The risk associated with the loss of privacy and confidentiality due to personally identifiable information that may be associated with specimens.
Common questions involving research using human specimens are summarized below.
Question: What type of IRB review is required for a research project using existing specimens? What HIPAA form do I need to submit?
Answer: It depends on whether the existing specimens are identifiable. Existing specimens means the specimens were collected for clinical purposes or for research studies other than the proposed research study.
If the existing specimens are not identifiable, and if the investigator will make no effort to re-identify the specimens, the specimens do not meet the definition of a human subject and IRB review would not be required.
On the other hand, if the specimens are identifiable, or efforts will be made to re-identify the samples, IRB review is required.
Research that only involves the use of existing identifiable specimens may qualify for exemption if one of the following is true:
- the specimens are publicly available
- Information is recorded in such a manner that the identity of the human subject cannot readily be ascertained directly or through identifiers linked to the subjects, the investigator does not contact the subjects, and the investigator will not re-identify subjects. In this case, the research may qualify for exempt status under Category 4.ii.
To address HIPAA submit a HIPAA Certification of De-Identification.doc
On the other hand, research involving previously collected specimens that have identifiers associated most likely qualifies for expedited review under category 5. Use of specimen-associated identifiers must be restricted and privacy protection measures must be in place.
To address HIPAA submit HIPAA Request for Alteration or Waiver of Authorization.doc
Question: What type of IRB review is required for a research project using specimens that will be collected for research purposes by noninvasive means? What HIPAA form do I need to submit?
Answer: Research that involves the collection of specimens for research purposes by noninvasive means may qualify for Expedited review- under Category 3.
Examples of these noninvasive collections of specimens are:
- Hair and nail clippings in a non-disfiguring manner
- Deciduous teeth at time of exfoliation or if routine patient care indicates a need for extraction
- Permanent teeth if routine patient care indicates a need for extraction
- Excreta and external secretions (including sweat)
- Un cannulated saliva collected either in an unstimulated fashion or stimulated by chewing gum base or wax or by applying a dilute citric solution to the tongue
- Placenta removed at delivery
- Amniotic fluid obtained at the time of rupture of the membrane prior to or during labor
- Supra‑ and subgingival dental plaque and calculus, provided the collection procedure is not more invasive than routine prophylactic scaling of the teeth and the process is accomplished in accordance with accepted prophylactic techniques
- Mucosal and skin cells collected by buccal scraping or swab, skin swab, or mouth washings
- Sputum collected after saline mist nebulization.
You will need to submit a HIPAA Authorization to Use and Disclose PHI for Research Purposes.doc
Question: What type of IRB review is required for a research project using specimens collected for research purposes by invasive means? What HIPAA form do I need to submit?
Research that involves the collection of specimens for research purposes by invasive means/using procedures that pose greater than minimal risk to participants must undergo full committee review by the IRB.
Examples of these invasive collections of specimens are:
- Collection of specimens through a skin Biopsy
- Collection of specimen through a bronchoscopy, amniocentesis or colonoscopy.
You will need to submit a HIPAA Authorization to Use and Disclose PHI for Research Purposes.doc
Question: My research study involves collecting sputum and lung aspirates from clinical procedures involving chronic smokers that are otherwise going to be thrown away. The specimens will be provided by the pathology department without identifiers. The pathologist will not be involved in the research. Do I have to get IRB review? If so, what HIPAA form do I need to submit?
Answer: You do not need to submit an application for IRB review nor you need to submit a HIPAA form. Your research is considered secondary research that is not human subjects research because: (a) the specimens were originally collected for clinical care and not specifically for the purpose of the investigator’s current research, (b) the specimens do not come with individually identifiable information, and (c) there is no interaction or intervention done specifically for the research.
| Section D- Questions related to the Privacy Rule & Recruitment Activities |
The IRB may approve a research proposal in which an investigator will obtain information for the purpose of screening, recruitment or determining the eligibility of prospective subjects without the prospective subject’s HIPAA authorization, however the following conditions must be met:
- The investigator will obtain information related to screening, recruiting or determining eligibility through oral or written communication with the prospective subject.
- The investigator will obtain identifiable information or identifiable biospecimens for screening, recruiting or determining eligibility by accessing records or stored identifiable biospecimens.
- In order to access records or specimens for such purposes, there must be an established relationship between the investigator and the individuals whose records /specimens will be reviewed. The investigator may delegate the review to designated UConn Health research staff.
Question: At what point in recruitment may we gather information about a potential participant (e.g., if a potential participant calls our office after seeing a flyer, may we screen that person/ ask them about their history, or do we need the person to complete a written HIPAA Authorization prior to screening)?
Answer: If the IRB has approved your recruitment plan, including a partial waiver of Authorization to permit you to collect PHI for screening without written Authorization, you may take the person’s contact and screening information. Investigators must also submit to the IRB a phone script using the Sample Phone Script for Screening Prior to Consent.doc . The IRB must approve the script prior to collecting information from potential participants over the phone.
The potential participant should know that in order to evaluate whether he or she is a candidate for the research, the researcher will need to share the caller’s information, and the caller may need to share information, with a limited number of others who staff the study. If the person is deemed qualified for the study, then he/she will be asked to come in to sign an informed consent and a HIPAA Authorization. To protect the privacy of the potential participant all the information they provide will be kept only if he/she qualifies to proceed and decides to participate in the study.
| Section E- Questions Related to HIPAA Identifiers and Coded Data/Specimens |
Question: HIPAA specifies18 identifiers that must be removed to “de-identify” health information. Is any one of these identifiers, all by itself, PHI?
Answer: Not necessarily. PHI is information, including demographic information, which relates to (i) the individual’s past, present, or future physical or mental health or condition; (ii) the provision of health care to the individual; or (iii) the past, present, or future payment for the provision of health care to the individual, and that identifies the individual or for which there is a reasonable basis to believe can be used to identify the individual. If the only identifier you have is a DOB and that DOB is not linked to any other health information and could not be sourced to a provider (e.g., UConn Health), the DOB alone would not be PHI. However, if the DOB is coupled with other information, such as “a patient at UConn Health,” or “was one of 15 enrollees in a particular study,” this combination would be PHI.
Question: What coded information or coded specimens means?
The Office of Human Research Protections (OHRP) has defined coded as:
- identifying information (such as name or social security number) that would enable the investigator to readily ascertain the identity of the individual to whom the private information or specimens pertain has been replaced with a number, letter, symbol, or combination thereof (i.e., the code);
and
- a key to decipher the code exists, enabling linkage of the identifying information to the private information or specimens.
OHRP considers the term investigator to include anyone involved in conducting the research. OHRP does not consider the act of solely providing coded private information or specimens (for example, by a tissue repository) to constitute involvement in the conduct of the research. Note that if the individuals who provide coded information or specimens collaborate on other activities related to the conduct of this research with the investigators who receive such information or specimens, then OHRP would consider such additional activities to constitute involvement in the conduct of the research.
Examples of such additional activities include, but are not limited to:
(1) The study, interpretation, or analysis of the data resulting from the coded information or specimens; and
(2) Authorship of presentations or manuscripts related to the research.
Question: Is coded information identifiable?
Answer: The Privacy Rule considers coded information to be de-identified if the 18 specific identifiers of the individual or of relatives, employers, or household members of the individual, listed below are coded and the person cannot reasonably be identified.
However, that code needs to be assigned by someone other than the investigator. The code cannot be derived from any identifiable piece of information or combination of pieces of identifiable information. The key to the code cannot be accessible to the investigator or research personnel using the de-identified data.
- Names;
- Address (including street address, city, county, zip code). The initial three digits of a zip code may be used if, according to the current publicly available data from the Bureau of Census: 1) the area formed by combining all zip codes with the same three initial digits contains more than 20,000 people; and 2) the initial three digits of a zip code for a region containing 20,000 or fewer people is changed to 000;
- All elements of dates (except year) for dates directly related to an individual (birth
- date, admission date, discharge date, date of death), and all ages over 89 and all elements of dates (including year) indicative of such age, except that ages and elements may be aggregated into a single category of age 90 or older;
- Telephone numbers;
- Fax numbers;
- Electronic mail addresses;
- Social Security numbers;
- Medical record numbers;
- Health plan beneficiary numbers;
- Account numbers (bank, retirement, credit card, etc.);
- Certificate/license numbers;
- Vehicle identifiers and serial numbers, including license plate numbers;
- Device identifiers and serial numbers;
- Web Universal Resource Locators (URLs);
- Internet Protocol (IP) address numbers;
- Biometric identifiers, including finger and voice prints;
- Full face photographic images and comparable images; and
- Any other unique identifying number, characteristic or code.
REFERENCES
HIPAA Privacy Rule and Its Impacts on Research (nih.gov)
- 2011-014.0.pdf– Health Insurance Portability and Accountability Act (HIPAA) in Research
HSPP Newsletter – July, August, September, 2023
HSPP Newsletter – July, August, September, 2023
Quality Improvement (QI) Projects & Human Subjects Research
When a project is planned with a goal of improving the performance of a departmental practice in relationship to an established standard, the activity is called quality improvement (QI).
Most quality improvement projects are not subject to the Department of Health and Human Services (HHS) regulations- the common rule. However, in some cases, quality improvement activities are designed to carry out a research study. In these cases, the regulations for the protection of subjects in research may apply.
To determine whether a quality improvement activity is also a human subject research project, the following questions should be addressed in chronologic order:
- Does the activity involve research?
- Does the research activity involve human subjects?
- Does the human subject research qualify for an exemption?
If the answer to the first or second question is no, the activity is only a QI project.
If the answers to each of the first two questions is yes, then the QI project is considered a human subject research project. The third question will be to determine whether your study will qualify for exempt status. If the research does not appear to qualify for exempt status, you will need to determine if it qualify for expedited or full board review.
If an investigator is not sure as to whether a QI project is also human subject research, it is recommended that a Human Subject Research Determination Form.doc be submitted to the IRB to obtain an official ruling before the activity commences.
When investigators submit a determination form, the IRB will evaluate multiple factors to make a determination. Some of the factors to be considered include, but are not limited to: the primary intent of the project. The IRB will consider the QI project a research study when the primary intent of the project is to produce generalizable results, or when the project will impose risks beyond the standards of care, and/or when the project includes randomization.
As an example of IRB considerations, the table below describes the IRB questions to determine whether an educational project is only a QI project.
When a QI project in an educational setting is part of a formal curriculum and participation in such project is not a choice, the activity will be considered only QI as long as the results of the project will only be shared with the program/department implementing the QI project.
On the other hand, when a QI project in an educational setting is not part of a formal curriculum and participation in such project is voluntary, the activity will be considered human subjects research as long as the results of the project will be shared outside of the institution implementing the QI project.
| Guidelines for Determining Whether Educational Activities are Quality Improvement Projects or Exempt Research | ||
| QI | Exempt Review | |
| Is the educational activity part of the formal curriculum (i.e., it would be offered/required regardless of the evaluation)? | Yes | No |
| Is the activity designed to continuously improve the quality of an educational offering? | Yes | No |
| Is there an intent to share the results beyond that department/program that is offering the educational activity? | No | Yes |
| Is participation in the evaluation of the educational activity voluntary? | No | Yes |
If investigators self-determine that IRB review is not necessary for a proposed project, they need to know that IRB approval cannot be granted retrospectively. In addition, federal regulations have made it clear that any publication describing a project as “research” must have received prior IRB review and approval.
Example of a Quality Improvement Project
At the time of patient registration existing hospital policy requires data points A, B and C to be collected. The patient registration center implements use of a registration template form to improve collection of data points A, B, and C. Six months later the patient registration data is analyzed to see if use of the form improved collection of the required data points.
Research Consideration: there is no hypothesis or experimental question being asked so the definition of “systematic investigation” is not met and therefore the definition of research is not met; and the intention is to improve compliance with an existing and accepted policy not to contribute to generalizable knowledge.
HIPAA Consideration: HIPAA allows for conducting quality assessment and improvements activities related to health care operations provided that the obtaining of generalizable knowledge is not the primary purpose. The minimum necessary information should be used.
To learn more about how the DHHS views quality projects in relation to the regulations for human subjects research please click on Quality Improvement Activities FAQs | HHS.gov
Human Subjects Protection Training through the Collaborative Institutional Training Initiative (CITI)
Frequently Asked Questions
I am submitting an application for Exempt Status. Do I need to complete Human Subjects Protection Training? If so, why?
Training of study personnel is required regardless of whether the research qualifies for exempt, expedited or full board review, or whether the facilitated review process is utilized.
I am a new UConn Health investigator. What is the CITI Training I should complete?
All key study personnel listed on an IRB application for either an initial submission or a request for modification must have a current/valid training in the protection of human subjects.
Investigators who are completing human subjects training for the first time should first select the user group most applicable to the type of research with which they will be involved. Prior to enrolling in any CITI Training course, the Investigators should respond to the CITI course enrollment questions within the CITI program also posted in the IRB website page.
UConn Health IRB Requirements for new investigator/new affiliated staff are as applicable: the Basic or Refreshment course of (1) Biomedical Investigators and Study Personnel, (2) Social and Behavioral Investigators and Study or (3) Students.
Investigators who are renewing their training, can select the Good Clinical Practice course to satisfy the requirements.
I am adding an external investigator to my study. Does he/she needs CITI Training? If so, what is the training course this investigator should complete?
As per IRB policy 2011-023.0.pdf – Educational Requirements, if an investigator is external to the UConn Health, they must submit proof of having completed human subjects protection training. These certificate can either be sent to cagganello@uchc.edu or be attached to the submission. The Training certificates submitted will be evaluated by the IRB staff to verify that the courses completed are the required by UConn Health IRB.
The IRB reserves the right to require the external investigator to complete additional training.
I completed my CITI Training a while ago, how can check if my CITI Training is up to date?
The IRB has a webpage dedicated to Human Subjects Training. Investigators or coordinators in need of checking CITI Training status for themselves of others may access the master training list.xlsx (Excel) which is updated approximately every two weeks.
In addition, investigators iRIS account are updated within 1-2 weeks with the CITI Training Reports. To check the status of your CITI training in iRIS you can complete these steps: Click on “My Assistant” Menu, and then click on “My Account Information” sub-menu. Go to the menu titled– Training History. You will be able to see your Courses Completion and Expiration date.
I would like to complete a refresher course in the CITI Program. However, the system prompts me to complete a Basic course. What can I do to complete a refresher course?
You need to complete the course that is due according to your previously completed course work. The CITI Program has been set to require the users to complete a refresher course only when the last completed course of the chosen group was a Basic course. This is required because the information in the modules is updated constantly and a basic course is the only venue to learn the new information. See example of a course completion history below.
Integrated Research Information System (iRIS)
Frequently Asked Questions
Who needs to request an account to access iRIS?
Investigators with an email address ending in ——@uchc.edu should not request an account in iRIS since they already have an account in iRIS. These investigators are considered internal investigators. As stated in the iRIS logging page the investigator’s UConn Health network username and password are to be used to log in to iRIS.
On the other hand, individuals who need access to iRIS but are not affiliated to UConn Health /do not have an UConn Health username and password (e.g., a Hartford Hospital clinician) need to request an account in our iRIS system. An online request form must be completed by clicking on the Request New Account option found in the iRIS logging page. To avoid inaccurate information this online request form should be completed by the person in need of the account.
I need to add an UConn Health investigator to my study. However his/her name is not found in the iRIS data base. Should this investigator request an account in iRIS?
As stated in the previous FAQ, internal investigators do not need to request an account in iRIS. You can search for the investigator’s name either in the iRIS database or in the LDAP directory.
The iRIS data base contains the names/accounts of investigators who have logged into iRIS at least once. If the internal investigator you are trying to add has never before logged in to iRIS, his/her name/account will not be found in the iRIS database.
The LDAP directory contains names/accounts of those investigators who have not logged into iRIS ever. Therefore, when you are trying to find the account of an internal investigator you should search in the LDAP directory.
I am having trouble logging into iRIS. Can I retrieve my iRIS logging credentials from the iRIS submission system?
If you are an Internal Investigator, iRIS does not storage internal users passwords.
Your current network ID and password should allow you to gain access to the system. If you know your password is active, go to https://imedris.uchc.edu and use your network ID and PW to log into IRIS (use the same ID and PW you use to access your UConn Health email account).
If you are still experiencing problems using your UConn Health credentials, please contact the UConn Health help desk at 860-679-4400.
If you are an External Investigator, and you do not remember your iRIS ID, send an email to cagganello@uchc.edu requesting your iRIS ID.
If you need to retrieve your password follow click on the “I forgot my Password” tab found in the iRIS logging page. Enter your iRIS User ID in the box provided. Then click on the “Send Password” tab. The IRIS system will send your password to the e-mail address found in your iRIS account.
If you are still experiencing problems using your credentials, please call 860-679-8802 or email cagganello@uchc.edu
I am an external investigator with an account in iRIS. I need to change the email address in my iRIS account. How can I do that?
To edit the email address noted in your iRIS account you will need to log into your iRIS account. Once you have logged into iRIS, complete the following four steps. Click on “My Assistant” Menu, then click on “My Account Information” Sub-menu. The system will open your Profile. In there you can edit your email address. To save the changes, click on the Save Section icon.
Investigators can also download the External Users- iRIS User Manual’s Instructions to Change Your Password & Email address from the iRIS help icon found in their iRIS Homepage.
U.S. Federal & Drug Administration (FDA) Warning Letters
FDA warning letter to Angela M. Stupi, Clinical Investigator
The investigator was cited for failing to ensure the investigation was conducted according to the investigational plan [21 CFR 312.60]
Failure to ensure that subjects met eligibility criteria before enrollment in the study.
Failure to ensure that the study drug was administered to subjects in specific body locations as required by the protocol
The warning letter also goes over how the clinical investigator’s written response did not provide sufficient details about their corrective action plan.
FDA warning letter to Randy Epstein, Clinical Investigator (Sponsor)
The investigator was cited for conducting research on an investigational drug without an IND, as well as failure to maintain adequate records showing the receipt, shipment, or other disposition of the investigational drug.
The warning letter goes over how the clinical investigator’s written response did not provide adequate corrective action plans.
FDA warning to Mobeen Mazhar, Clinical Investigator
The investigator was cited for failing to ensure the investigation was conducted according to the investigational plan [21 CFR 312.60], and failure to obtain informed consent in accordance with the provisions of 21 CFR part 50 [21 CFR 312.60 and 21 CFR 50.20].
Educational Resources for Investigators
Office of Human Research Protection (OHRP) Webinars on 45CFR46
The Office of Human Research Protection has posted the following webinars recordings and slides:
Respecting Persons- From Basic Requirements to Embracing Participant- Centered Informed Consent
This presentation reviewed ethical principles, discussed regulatory requirements for informed consent, and offered strategies to develop high-quality, participant-centered informed consent documents and discussions.
Unlocking the Mysteries of the §46.111 Criteria for IRB Approval of Research
This presentation explains the criteria for IRB approval of research and includes case studies and interactive quizzes to demonstrate the way the criteria can be applied.
Access Video here
Doing Research with Data and Biospecimens under the Common Rule Part 1 – What Researchers should know
This presentation explained how the Common Rule applies to secondary research with data and biospecimens.
Doing Research with Data and Biospecimens under the Common Rule Part 2 – How Does that work with Repositories and Future Use
This presentation explained how the Common Rule applies to research repositories.
HSPP – April-May-June, 2023 –Newsletter
The Association for Accreditation of Human Research Protection Programs
UConn Health Human Subjects Protection Programs Preparation for Reaccreditation
The Association for Accreditation of Human Research Protection Programs (AAHRPP) is an independent, non-profit accrediting body that works to protect the rights and welfare of research participants and promotes high-quality research through an accreditation process.
AAHRPP’s accreditation standards meet or exceed U.S. federal regulatory requirements and the International Committee on Harmonisation –Good Clinical Practice (E6) guideline for protection, and are reasonable, attainable, and representative of current best practices.
UConn Health’s Human Subjects Protection Program (HSPP) achieved AAHRPP accreditation in 2006. As an accredited organization, our HSPP must periodically apply for re-accreditation every five years. This is a two-step process.
Step 1, consists of a self-evaluation of our program, followed by an AAHRPP review of our policies and procedures to ensure they meet regulatory and accreditation standards.
Step 2 is an onsite visit by AAHRP representatives to ensure that our policies and procedures are followed. Once our HSPP is scheduled for the reaccreditation visit an announcement will be sent to the research community.
To complete the reaccreditation step 1, the HSPP has revised multiple IRB policies to reflect our current practices, add required information and standards for accreditation.
In the tables below is a list of the IRB polices and forms that have been revised along with a short summary of the revisions.
If you have questions regarding those changes please send an email to either irb@uchc.edu or contact the Education Specialist at cagganello@uchc.edu , 860-679-8802.
2009-001.0.pdf – Reporting Unanticipated Problems to the Institutional Review Board: Edited section under “Self-Reporting” to clarify that the Principal investigators are to report to the IRB any noncompliance with the protocol or directives of the IRB that was within the control of the research team within 5 business days of becoming aware of the event.
2009-003.0.pdf – Imposing and Lifting Suspensions of IRB Approval or Imposing Terminations of IRB approval: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2009-005.0.pdf – Monitoring of IRB Approved Studies: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-006.1.pdf – Additional Protections – Pregnant Women, Fetuses or Neonates: Minor grammar changes.
2011-006.4.pdf – Additional Protections – Other Vulnerable Groups: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-006.5.pdf – Additional Protections – Fetal Tissue Transplants: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-007.0.pdf – Definitions Applied to Policies: Added definition of benign behavioral intervention. Edits to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their). Included revised common rule.
2011-008.1.pdf – Informed Consent – Process The general section was revised to request information about the informed consent methods and documentation and to alert the investigator that prospective IRB approval is required for any subsequent modifications made to the methods of obtaining consent or documentation of informed consent whether they are done by hard copy or electronically.
- Changes to the process of obtaining consent by Phone / Fax to include that the individual obtaining consent must be approved by the IRB to consent and that such individual should have sufficient knowledge of the study to conduct the conversation and to answer any questions,; and the consent conversation should include an in-depth review of the consent document allowing sufficient time for questions to be asked and answered.
- The process for obtaining consent via videoconference (e.g., WebEx, Zoom) was added with an explanation of how this process must be conducted.
- A section about obtaining electronic documentation of consent was added with details of compliance expectations and acceptable methods and processes to obtain electronic signatures.
- A section about electronic informed consent process when consent is not witnessed by study personnel was added to alert researchers that the investigator planning to use this method should discuss this plan with the IRB prior to submitting this method for approval to ensure this method is appropriate for the research (e.g., in compliance with applicable regulations).
- Edits to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their).
2011-008.5.pdf – Informed Consent – Providing and Obtaining Informed Consent: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-009.0.pdf– Institutional Review Board – Membership: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-009.11.pdf – Institutional Review Board – Studies Conducted in Foreign Locations: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-009.14.pdf – Institutional Review Board – Human Subject Research Determinations: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-009.2.pdf – Institutional Review Board – Exemptions: Policy was edited to remove language related to pending adoption of the revised common rule and revisions to applicability of exemption 4(iii) at UConn Health.
2011-009.3.pdf – Institutional Review Board – Expedited Reviews : Policy was revised to include a complete list of the criteria for approval when conducting initial or continuing review for expedited submissions. In addition, when submissions are returned to the investigators with a status of “Approved Contingent,” the IRB reviewer can now add a deadline for the investigator to respond to the contingencies sent in a Response form.
2011-009.4.pdf – Institutional Review Board – Convened Meeting Operations: Policy was revised to add that when virtual IRB meetings are conducted the agenda item (inclusive of supporting documents) are shared on the screen in the videoconference.
2011-009.7.pdf – Institutional Review Board – Assignment of Status Codes: Policy was revised to clarify the IRB will assign the study status code “Closed by PI” to a study under oversight of an external IRB when the external IRB grants the request. Under the status code title: “Inactive-Administratively Closed” the following was added: the IRB Administrator will assign this status code to exempt research after the anticipated completion date has passed.
2011-009.8.pdf – Institutional Review Board – Appeals Process: Policy was revised to indicate that when a principal investigator (PI) submits an initial appeal letter, it can be completed through a written correspondence (i.e., not limited to IRIS response). Also, the letter sent by the IRB in response to the appeal made by the PI will contain a wet-ink or electronic signature of the IRB Chair. In addition some edits were made to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their).
2011-009.10.pdf – Institutional Review Board – More Frequent Review: Policy Appendix -A was revised to remove Panel 3 and CICATS.
2011-009.12.pdf – Institutional Review Board – Criteria for Approval: Policy was revised to clarify that students can be considered subjects who are likely to be vulnerable to coercion or undue influence. In addition, policy revised to remove language indicating ‘if’ the revised common rule is implemented (see section describing limited IRB review).
2011-009.13.pdf – Institutional Review Board – Lapse in IRB Approval: Policy was revised to describe that investigator are notified either by email or iRIS correspondence about the need to submit a request for extension of the anticipated completion date or close the study.
2011-009.15.a.pdf – Institutional Review Board – Reliance on UConn Health as IRB of Record: Policy was revised to indicate SMART IRB template may be used to execute reliance agreements. The Office of Human Research Protection reliance agreement template was removed as it not preferred since it does not meet AAHRPP standards.
2011-009.15.b.pdf – Institutional Review Board – Reliance on External IRB: Trinity Health was added as an institution with which UCONN Health has an established collaborative agreement for minimal risk studies conducted by a student, fellow or resident. Also, policy now contains that when requesting reliance on an external IRB for a student/resident/fellow project, UCONN Health IRB may request the original approval letter to ensure the research is minimal risk.
2011-011.0.pdf – Research Personnel: Policy revised to include principal investigator (PI) responsibility to ensure the confidentiality and security of research records and data as described to the IRB in the submission materials, and to cooperate with all aspects of internal or external audits and inspections.
2011-012.0.pdf – Conflict of Interest – Research Personnel: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-012.1.pdf – Conflict of Interest – IRB Members: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-015.0.pdf – Recruitment and Payment: Policy was revised to indicate that external researchers looking to advertise recruitment in UConn Health broadcast (e.g., Lifeline) messages do not need HSPP/IRB permission. Also revised to include procedure to use UConn Health as a recruitment site when UConn Health is not engaged. Added edits to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their).
2011-016.0.pdf – Scientific Review: Policy was revised to include the Clinical Research Center and funding foundation as acceptable entities who may have conducted the scientific review of studies submitted for full board review.
2011-020.0.pdf – Humanitarian Use Device: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-022.0.pdf – Study Drug – General: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-022.2.pdf – Investigational Drug/Biologic – Expanded Access for Treatment Use, Including Single Emergency Use: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-023.0.pdf – Educational Requirements: Updated to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their) and minor punctuation and grammar changes.
2011-025.0.pdf – HSPP Evaluation / Institutional Support: Policy was revised to include minor updates to title of HSPP manager, and removing executive committee.
2014-034.0.pdf – Additional Requirements – Department of Education (Federal): Policy was revised to include that an email confirming with all of the information included in the FERPA verification form may be acceptable, provided the email is from the person at the school with the authority to grant the permission and sent from that individual’s institutional email address. Added edits to reflect current guidance on diversity, equity and inclusion (change he/she to they, his/her to their).
Application Checklist for Initial Exempt Application .doc: Exempt submission checklist Added the following requirements: When submitting for Exempt determination under Exempt category 4.iii a confirmation that the data will remain protected under HIPAA for 4.iii is required. If the protocol involves sharing data with indirect identifiers such as sharing a Limited Data Set with an external investigator the UConn Health investigators should provide confirmation they have in place a Data Use Agreement. If the protocol involves sharing coded data the UConn Health investigators should provide confirmation they have a Don’t Ask /Don’t Tell agreement in place.
Application Checklist for Initial and Continuing Review Expedited .doc : Expedited submission checklist Added the following requirement:
When using electronic informed consent (eIC) (confirmation of part 11 compliance, hard copies of materials, access to eIC platform)
Application Checklist for Initial and Continuing Review Full Board.docx
Application Checklist for Initial and Continuing Review Full Board.docx : Added the following requirement : When using electronic informed consent (eIC) (confirmation of part 11 compliance, hard copies of materials, access to eIC platform).
Request for Exemption Form .doc: Request for Exemption Category 4.iii. was revised to be less restrictive but still ensure HIPAA protection for review as required under the exemption.
Guidance on Closure of Human Subject Research Studies
A research study should be closed by the Principal Investigator (PI) once all human research activities are completed regardless of whether a study is subject to the continuing review requirement. To do so, a closure form should be submitted to the IRB through the iRIS submission system for each non-exempt human research study (e.g., studies approved under Expedited review or Full Board review). The closure form should be submitted before the expiration of IRB approval, however, the PI can also submit a closure form after they have received a notice of lapse of approval.
If the study is an exempt study, the PI may allow the IRB approval to expire. When approval of an exempt study expires, the IRB will administratively close the study, but this does not invalidate the exemption. The research, as proposed to the IRB, may continue; it is not necessary to keep the exemption actively registered with the IRB.
A closure form allows the IRB to have a summary of the following information:
• the findings of the study
• the final enrollment data
• whether the study met the recruitment goals, and
• whether any of the following events occurred since the last approval (initial or continuing review):
o subject complaints
o unanticipated problems involving risk to subjects or others,
o unexpected profile of adverse events in terms of frequency and/or severity,
o non-compliance with or deviation from the approved protocol or procedures,
o audits, inspections or monitoring visits by internal or external personnel.
o any publications, presentations, trademarks, patents, etc. related to the study.
This guidance explains the circumstances in which a non-exempt human research study may be closed from IRB oversight, as well as ongoing researcher responsibilities that apply to closed studies.
Things to Consider before Closing Research Studies
• Investigators should honor wishes of the sponsor or funding source to keep the study open or to close the study. Some funding entities require IRB approval for the duration of the funding, even if human research activities are complete, or they may not allow the study to close without the sponsor’s permission. It is the PI’s responsibility to be aware of, and comply with, those requirements.
• Sponsors, contract research organizations (CROs), or coordinating center personnel may need to verify or monitor individually identifiable study data at a specific site where human subjects activities have been completed. The study team should verify whether these organizations require the studies to be open when conducting their monitoring visits. IRB approval must be maintained while these activities are occurring.
• Whenever possible, prior to closing a study, data should be permanently de-identified.
When to Close a Study
• For studies requiring continuing review (e.g., some Expedited studies and all full board studies ) a requests for closure should be submitted at the time the next continuation application is due or within 30 days after the completion of all study activity involving the use of private identifiable information or biospecimens, whichever comes first.
• Moreover, a closure form should be submitted to the IRB if the if the research study was not conducted or was canceled, or if each of the following conditions exist:
o The research is permanently closed to the enrollment of subjects
o The subjects have completed all research-related interventions
o The research is no longer active for long-term follow up of subjects
o Data has been de-identified.
• When a Principal Investigator terminates employment with UConn Health, the PI may submit a closure form to the IRB. Alternatively, the PI may submit a modification form requesting transfer of the study to another eligible Principal Investigator.
Retired investigators with Emeritus status at UConn Health may be permitted to keep the study open and continue as the PI with approval from the HSPP Director.
• When a student-led project is completed, the study should be closed with the IRB. This should occur prior to the student’s departure / graduation.
IRB Process of Expired studies, Lapsed Studies and Closure Forms
• Expired studies: If approval for continuation of non-exempt research is not sought, or a request to extend the expected completion date has not been received within a reasonable time frame (e.g., 30 days), IRB staff will administratively close the study and send a written notification to the Principal Investigator of the administrative closure. The research activity may not continue and a new application may be required to resume research activity.
• Lapsed studies: If approval of the study has lapsed due to lack of a response to contingencies or a request for continuing approval or to extend the completion date has not been received the study may administratively be closed. The IRB will send a written notification to the PI. Prior to closure the IRB will issue a final request for response by email to the PI and study contacts and the PI will be given a reasonable period within which to respond (e.g. one or two weeks).
• Closure forms: When a closure form is submitted, the IRB will review any new information provided in the closure form and determine whether any additional action is required on the part of the IRB or the investigator. Upon review of the closure form, the status of the study is changed in the iRIS system (e.g., “Closed by PI”) and an outcome letter is issued confirming the closure.
Principal Investigator Responsibilities with Closed Studies
The principal investigator (PI) continues to have responsibilities for a study even when IRB oversight of a study is no longer required. These responsibilities include:
• Verifying all research activities have been completed. The PI should ensure that all research-related activities, interventions or interactions with human subjects or individually identifiable data have been completed at the site(s) approved under the Principal Investigator’s IRB application at the time a closure form is submitted to the IRB or at the time of approval expiration, whichever occurs first.
If after a study is closed, the PI wishes to engage in an activity such that the criteria for closure listed above would no longer be met, the Principal Investigator must submit a new application for IRB review and approval for the use of the previously collected data.
• Record Retention Research data from the completed study should be stored and protected in the manner approved by the IRB and consented to by the research participant so as to maintain the privacy and confidentiality of the participants.
Per HSPP Policy 2011-024.0.pdf – File Requirements & Record Retention Requirements , investigators must maintain research records for three years beyond the completion/termination of the study. Investigators should be aware that other laws and requirements (e.g., funding agency) may require a longer record retention period. Per the HIPAA regulation, investigators are to retain documents relating to uses and disclosures, authorization forms for 6 years from the date of creation or the date when it last was in effect, whichever is later.
Investigator should be familiar with the record retention format described in the UConn Health HSPP Policy 2015-024.1.pdf – Record Retention Format .
Investigators should ensure that any specific regulatory and/or sponsor requirements are met for record retention or submission of reports.
• Confidentiality and Data Security. If the PI is maintaining identifiable private data or specimens, the protections described in the IRB application and to subjects must be maintained for the time frame described. The PI must continue to honor any commitments made to participants as part of the approved research (e.g., providing information about study results; payment for research participation).
• HIPAA authorization. The PI may have obtained HIPAA authorization from subjects to access their medical records, with an expiration date that is far in the future. If the PI still has permission to access medical records at the time they want to close the study that permission expires upon study closure.
U.S. Department of Health and Human Services Food and Drug Administration
Common Inspection findings from 2017-2022
The Food and Drug Administration (FDA) has released their Bioresearch Monitoring (BIMO) Fiscal Year 2022 Metrics. Below is a partial description of the common inspection findings from 2017-2022. The full report can be found here: https://www.fda.gov/media/165853/download
Common Sponsor-Investigator Inspectional Observations:
• Failure to maintain and/or retain adequate records in accordance with 21 CFR 312.57; accountability for the investigational product; Investigator Statement (FDA 1572); Financial disclosures.
• Failure to select qualified investigators and/or monitors, ensure proper monitoring of the study and ensure the study is conducted in accordance with the protocol and/or investigational plan.
• Failure to submit an Investigational New Drug (IND) application.
• Inadequate subject protection; informed consent issues.
• Failure to notify FDA of termination of investigator.
Common Sponsor/CRO Inspectional Observations:
• Failure to ensure proper monitoring of the study and ensure the study is conducted in accordance with the protocol and/or investigational plan.
• Failure to meet the abbreviated requirements for investigational device exemptions (IDEs).
• Failure to maintain and/or retain adequate records in accordance with 21 CFR 312.57; accountability for the investigational product; Investigator Statement (Form FDA 1572); Financial disclosures.
• Failure to submit an Investigational New Drug (IND) application; IND safety report.
• Failure to submit current list of all participating investigators to FDA at six-month interval after FDA approval of the study.
Common Clinical Investigator Inspectional Observations:
• Failure to comply with Form FDA 1572 requirements, protocol compliance
• Failure to follow the investigational plan; protocol deviations
• Inadequate and/or inaccurate case history records; inadequate study records
• Inadequate accountability and/or control of the investigational product
• Safety reporting; failure to report and/or record adverse events
• Inadequate subject protection; informed consent issues
Difference Between De-Identified Data Sets and Limited Data Sets
&
Limited Data Sets and Data Use Agreements
Under the Health Insurance Portability and Accountability Act (HIPAA) de-identified data is data from which all 18 HIPAA identifiers that could be used to identify an individual or the individual’s relatives, employers, or household members have been removed.
Unlike a de-identified data set, a limited data set is still considered Protected Health Information (PHI). As defined by HIPAA, limited data sets (LDS) are data sets stripped of certain direct identifiers that are specified in the Privacy Rule. They are not de-identified information under the Privacy Rule.
A limited data set is protected health information that excludes the following direct identifiers of the individual or of relatives, employers, or household members of the individual: (1) names; (2) postal address information, other than town or city, State, and zip code; (3) telephone numbers; (4) fax numbers; (5) e-mail addresses; (6) social security numbers; (7) medical record numbers; (8) health plan beneficiary numbers; (9) account numbers; (10) certificate/license plate numbers; (11) vehicle identifiers and serial numbers; (12) device identifiers and serial numbers; (13) web URLs; (14) Internet Protocol (IP) address numbers; (15) biometric identifiers, including fingerprints and voiceprints; and (16) full-face photographic images and any comparable images.
Distinct from de-identified data, a limited data set contains protected health information that is associated with indirect identifiers as defined in the HIPAA privacy rule. Protected health information in limited data sets may include the following indirect identifiers: town, city, state and zip code, and dates directly related to an individual, including birth date, admission date, discharge date and date of death.
The table below describe in detail the HIPAA identifiers that must not be present in a de-identified data set or in a limited data set.
| DATA ELEMENT | DE-IDENTIFIED DATA SET | LIMITED DATA SET |
| Names. | Remove | Remove |
| Postal address information. | Remove | Remove |
| Town, city, state and zip code. | Remove | Can retain city, town, state or full zip code. |
| All elements of dates that are directly related to an individual, including birth date, admission date, discharge date, death date, and all ages over 89 and all elements of dates (including year) indicative of such age, except that such ages and elements may be aggregated into a single category of age 90 or older. | Remove | Remain |
| Telephone numbers, fax numbers; e-mail addresses, web URL addresses, IP addresses. | Remove | Remove |
| Social security number, medical record number, health plan beneficiary number, any account number, certificate or license number. | Remove | Remove |
| Vehicle identifiers and serial numbers, including license plate numbers, Device identifiers and serial numbers. | Remove | Remove |
| Full-face photographic images and any comparable images, Biometric identifiers, including fingerprints and voiceprints. | Remove | Remove |
| Any other unique identifying number, characteristic or code. | Remove | Remove |
Limited Data Sets and Data Use Agreements
If indirect identifiers must be kept within a limited data set (LDS) in order to perform a research study and the information is to be disclosed outside of UConn Health, the principal investigator must enter into a Data Use Agreement (DUA) with the data recipient. A DUA may also be utilized when UConn Health is the recipient of a LDS. Only after the agreement has been executed can the limited data set be used/disclosed.
This DUA is required under the HIPAA Privacy Rule. This agreement establishes the ways in which the information in the limited data set may be used, the purpose for which it was disclosed, and identifies who is permitted to use or receive the information.
Moreover, the DUA stipulates that the recipient will use appropriate safeguards to maintain the confidentiality and protect the data from further disclosures.
Since the data use agreements establish institutional obligations and bind the institution to the terms of the agreement, investigators are not authorized to execute research DUAs. UConn Health DUAs for research related activities are processed through the Office of Sponsored Programs Sponsored Program Services (SPS) or the Office of Clinical and Translational Research (OCTR). The specific contacts in these offices are listed below:
• If the DUA is related to a Clinical Trial contact: Donald Deyo, Contract Specialist (deyo@uchc.edu), or the OCTR main inbox (octrclinicaltrial@uchc.edu).
• If the DUA is unrelated to a Clinical Trial contact: Jennifer Pomales pomales@uchc.edu
The table below describes whether IRB review approval is required for a de-identified data set or for a limited data set, and when a Data Use Agreement is required.
| DE-IDENTIFIED DATA SET | LIMITED DATA SET | |
| IRB Review/Approval | IRB and Investigator can determine the project /research is Not Human Subject research. May be used in any manner, not regulated under HIPAA. |
If the data is not readily identifiable, IRB can determine Not Human Subject Research. IRB does not require HIPAA Authorization or Waiver. |
| Data Use Agreement | Not required. | Required.
UConn Health DUAs for research related activities are processed through the Office of Sponsored Programs Sponsored Program Services (SPS) or the Office of Clinical and Translational Research (OCTR). |
OHRP’s Common Rule Webinar
Join the introduction-level, webinar titled “Unlocking the Mysteries of the §46.111 Criteria for IRB Approval of Research.”
This presentation will explain the criteria for IRB approval of research and include case studies and interactive quizzes to demonstrate the way the criteria can be applied.
Date: Tuesday, July 11, 2023, 12:00 PM EDT
Spots are limited. Registration is required to attend and receive a certificate of attendance.
Register for this webinar at: https://www.zoomgov.com/webinar/register/WN_9RbRyAwjQY2N_kRxFPbT-w
New NSF Responsible Conduct of Research Requirement— Effective 7/31/23
UConn Health is committed to maintaining the highest ethical standards in the performance, reporting, reviewing and proposing of research and scholarly activity. In support of this commitment and to fulfill funder requirements, UConn Health offers Responsible Conduct of Research (RCR) training and education with the goal of engaging researchers in the exploration of best ethical practices.
A recent National Science Foundation (NSF) requirement expansion includes RCR training for faculty and other senior personnel, and will require that the training address mentor training and mentorship. These new requirements apply to NSF proposals submitted on or after July 31, 2023.
A list of RCR trainings at UConn Health that fulfill NSF RCR requirements can be found on our UConn Health RCR webpage. Be on the lookout for additions to the RCR offerings in the coming months!
ClinicalTrials.gov Modernization Efforts
Let your voice be heard! ClinicalTrials.gov is getting a facelift and the National Library of Medicine wants your feedback.
The National Library of Medicine (NLM) is holding a virtual public meeting to discuss the ongoing modernization efforts for ClinicalTrials.gov on April 25th, 2023, from 12:30-3:00 p.m. They will provide a detailed look at the current beta websites–– both the public-facing ClinicalTrials.gov site as well as the entry system site for researchers, known as the Protocol Registration and Results System or PRS. They will provide progress updates and ask for feedback from stakeholders. For the meeting agenda and a link to register, visit the NLM website.
For questions regarding ClinicalTrials.gov at UConn and UConn Health, please contact local PRS Administrator, Ellen Ciesielski
NIH Plan to Enhance Public Access to the Results of NIH-Supported Research (NIH Public Access Plan)
The Office of the Vice President for Research would like to share some information with researchers who may be affected.
The National Institutes of Health (NIH) is hosting a virtual, public listening session next Wednesday, April 12, 2023, from 1:00 – 3:00 pm for feedback on the NIH Plan to Enhance Public Access to the Results of NIH-Supported Research (NIH Public Access Plan). The virtual listening session will be viewable through NIH Videocast. Further information about the listening session, including the agenda and how to sign up to make oral comments, can be found on the event page of the Office of Science Policy (OSP) website. The slots for oral comments will be provided in the order they are received until all slots have been filled, and must be received by April 10, 2023.
Written Request for Information (RFI) responses on the NIH Public Access Plan will continue to be accepted until April 24, 2023.
For questions, you can contact OSP at SciencePolicy@od.nih.gov.
HSPP- January-February -March, 2023 – Newsletter
HSPP- January-February -March, 2023 – Newsletter
Important Updates about the COVID-19
Single Institutional Review Board (IRB) Exception
Based on current COVID-19 trends, the U.S. Department of Health and Human Services (HHS) is planning for the federal Public Health Emergency (PHE) for COVID-19, declared under Section 319 of the Public Health Service (PHS) Act, to expire at the end of the day on May 11, 2023. The Office for Human Research Protections (OHRP) is sending this announcement in anticipation of the PHE expiration.
On October 8, 2020, OHRP, on behalf of HHS, issued an exception determination as permitted by 45 CFR 46.114(b)(2)(ii) stating that certain categories of cooperative research supported or conducted by HHS and subject to the 2018 Requirements are not required to comply with the single IRB mandate in 45 CFR 46.114(b)(1). The full text of the exception can be found here: https://www.hhs.gov/ohrp/regulations-and-policy/single-irb-exception-determinations/october-2020-exception-determination/index.html
Use of this exception is permitted for research that is ongoing or initially reviewed by the IRB during the COVID-19 public health emergency declared by the Secretary of HHS when reliance on a single IRB would not be practical and when the HHS division supporting or conducting the research approves the use of the exception. OHRP granted this exception due to the unprecedented burden and disruption to the research enterprise caused by the COVID-19 public health emergency, which also necessitated urgent research responses.
Institutions and IRBs should be cognizant of the impact that conclusion of the COVID-19 public health emergency will have on the ability to use this exception. Specifically, as of the date of the conclusion of the public health emergency, the exception will expire and cannot be applied to additional studies. Research for which the HHS division supporting or conducting the research study has already approved the use of the exception will continue to be excepted from the single IRB requirement, since the exception applies for the duration of the research.
Please direct questions to OHRP@hhs.gov or to the HHS division supporting or conducting a particular research activity.
An HHS fact sheet on the COVID-19 PHE transition roadmap can be found here: https://www.hhs.gov/about/news/2023/02/09/fact-sheet-covid-19-public-health-emergency-transition-roadmap.html
UConn Health Human Subjects Protection Program (HSPP)
External Research Use of UConn Health
External investigators (non-UConn Health personnel) who would like to conduct research recruitment activities at UConn Health which do not engage UConn Health, should complete and submit the Request for UConn Health as a Recruitment Site -Without Engagement and any approved recruitment materials to irb@uchc.edu.
External investigators who are in need of UConn Health resources for their research studies are to complete and submit the Confirmation of Available Resources Form (incl Inpatient Stays) . In this form, the investigator should describe all the resources that will be required for the research study. Completed forms and a copy of the approved protocol are to be submitted to irb@uchc.edu for approval by research and hospital administration. External protocols should describe the use of UConn Health as a research site. Researchers will need form approval in order to use resources at UConn Health for research.
Study Closures
Frequently Asked Questions
Q: When can I close my study with the IRB?
- If the study is an exempt study, the principal investigator (PI) may allow the IRB approval to expire. If so, the IRB will administratively close the study, which does not invalidate the exemption. The research, as proposed to the IRB, may continue. It is not necessary to keep the exemption actively registered with the IRB.
- If the study is a non-exempt study ( e.g., Expedited or full board studies) the PI can only close the study:
- If the research was not conducted or was canceled, or
- If each of the following conditions exist:
- The research is permanently closed to the enrollment of subjects
- The subjects have completed all research-related interventions
- The research is no longer active for long-term follow up of subjects
- Data has been de-identified.
Q: I am a Principal Investigator of an active /currently approved study. I am going to retire from UConn Health. Do I need to close my active studies?
- When a PI terminates employment with UConn Health, the PI should submit a modification form requesting transfer of the study to another eligible Principal Investigator. Alternatively, the PI may submit a closure form to the IRB.
- If the retired investigator has become an Emeritus professor for UConn Health, he/she can keep the study open and continue as the Principal investigator or co-investigator of the study. Approval from the HSPP Director is required in these cases.
Q: How do I close an IRB approved study?
- The PI should submit a Study Closure form through the iRIS system. The closure form should be submitted before the expiration of IRB approval.
- The investigator can also submit a closure form after he/she has received a notice of lapse of approval.
Q: How does the IRB process expired studies, lapsed studies and closure forms?
- When a closure form is submitted, the IRB will review any new information provided in the closure form and determine whether any additional action is required on the part of the IRB or the investigator. Upon review of the closure form, the status of the study is changed in the iRIS system (e.g., “Closed by PI”) and an outcome letter is issued confirming the closure.
- For non-exempt studies: if approval for continuation is not sought, or a request to extend the expected completion date has not been received within a reasonable time frame (e.g. 30 days), IRB staff will administratively close the study and send a written notification to the Principal Investigator of the administrative closure.
- For exempt studies: when approval has expired and a closure form has not been submitted, the IRB will administratively close the study. (see prior question about closure of exempt studies)
- For lapsed studies for which a response to contingencies has not been received within a reasonable time frame (e.g. 30 days) the study may administratively be closed. The IRB will send a written notification to the PI. Prior to closure the IRB will issue a final request for response by email to the PI and study contacts and the PI will be given a reasonable period within which to respond (e.g. one or two weeks)
Q: What are the expectations of the IRB with my closed studies?
- Ensure that all research-related activities, interventions or interactions with human subjects have been completed at the site(s) approved under the Principal Investigator’s IRB application at the time a closure form is submitted to the IRB or at the time of approval expiration, whichever occurs first.
- The PI will continue to maintain confidentiality protections of the data as outlined in the protocol, consent and IRB documents.
- Ensure that all subject identifiers connected with the research data have been destroyed in compliance with an approved Waiver of Health Insurance Portability and Accountability Act (HIPAA) Authorization (if applicable) and if the investigator indicated in the IRB application that all subject identifiers would be destroyed upon completion of the research.
- Retain research records in accordance with IRB Policies 2011-024.0.pdf – File Requirements & Record Retention Requirements and 2015-024.1.pdf – Record Retention Format.
- Ensure any specific regulatory and/or sponsor requirements are met for record retention or submission of reports.
- If after a study is closed, the investigator seeks to engage in an activity such that the criteria for closure listed above would no longer be met, the Principal Investigator must submit a new application for IRB review and approval for the use of the previously collected data.
Office of Human Research Protection (OHRP)
Short Videos – Educational Resources for Investigators
The Office of Human Research Protection has posted a series of short educational videos on research with private information and biospecimens. These videos are titled: “Regulatory Options for Secondary Research with Private Info and Biospecimens Part 1 and Part 2.”
Part 1 of these videos explains how to apply the regulations when doing research with data and/or biospecimens under the revised common rule.
This video discusses the concept of secondary research and how secondary research can be done under the revised Common Rule.
Definitions and examples of the following concepts are described in detail:
- What is secondary research and identifiable information.
- What is secondary research with nonidentifiable materials
- What is secondary research with identifiable materials
- Doing research with coded biospecimens and/or coded private information -When is human subject research?
Part 2 discuss how to address consent and HIPAA in a primary study when the investigator plans to share identifiable information for secondary research.
Investigators who watch the above videos should keep in mind that Exemption Categories 7 and 8 are not utilized at UCONN HEALTH.
Office of Human Research Protection (OHRP)
NIH Grants Conference in December 2022- Recording
The Office of Human Research Protection has made public the recording of a presentation provided last December 6, 2022 at the virtual NIH Grants Conference:
The presentation “ How Do I Know if a Research Study is Human Subjects Research and What Does that Really Mean? “ explains what makes a study “human subjects research” under the Common Rule, what responsibilities that entails, and what flexibilities may be available to simplify review for human research protections.
This presentation explains in detail our UConn Health Human Subject Research Determination Form.doc definitions and provides examples of research determinations.
UConn Health IRB Polices Revisions
The following UConn Health IRB Policies have been updated with language related to the 2019 revised common rule:
- 20112011-007.0.pdf– Definitions Applied to Policies (3/16/2023)
- 2011-006.2.pdf– Additional Protections – Prisoners (3/16/2023)
- 2011-008.0.pdf– Informed Consent – Forms (3/16/2023)
- 2011-008.2.pdf– Informed Consent – Waivers and Alterations (3/16/2023)
- 2011-008.4 .pdf– Informed Consent – Short Form (3/16/2023)
- 2011-009.3.pdf– Institutional Review Board – Expedited Reviews (3/16/2023)
Personnel Changes at the HSPP/IRB
New Research Compliance Monitor in HSPP: After working at UConn Health for many years as a research associate/coordinator, Rebecca Burke has joined our team as Research Compliance Monitor for the HSPP. You can reach Rebecca at burke@uchc.edu and 860-679-3054.
HSPP- October-November- December,2022 – Newsletter
FDA Warning Letter Regarding the Failure to Submit INDs for the Conduct of Clinical Investigations
with an Investigational Product that met the Definition of a Combined Product.
Inspections of clinical trials are conducted as a part of the U.S. Food and Drug Administration (FDA)’s Bioresearch Monitoring Program. These inspections are designed to evaluate the conduct of research and to help ensure that the rights, safety, and welfare of human subjects have been protected. Below you will find a short summary of a warning letter issued because of the failure to submit an investigational new drug application.
Warning Letter to Dr. David M. Lubeck/Arbor Centers for EyeCare
On November 18, 2022, the FDA issued a warning letter to Dr. David M. Lubeck/Arbor Centers for EyeCare. The FDA officials inspected Dr. Lubeck study and concluded that the investigator did not adhere to the FDA regulations governing the conduct of clinical investigations and the protection of human subjects. Specifically, the investigator failed to submit an Investigational New Drug application (IND) for the conduct of a clinical investigation with investigational new drugs that is subject to 21 CFR 312.2(a) [21 CFR 312.20(a), 312.20(b), and 312.40(a)].
The FDA argued that the investigational product used in combination with another drug comprised both a drug and a device components and was therefore a combination product within the meaning of section 503(g) of the FD&C Act (21 U.S.C. 353(g)).
Furthermore, the FDA underlined that because the primary mode of action of the investigational combination product was attributable to the product and because the product met the definition of a drug under section 201(g) of the FD&C Act, an IND was required for any clinical investigation of the investigational combination product used in such Protocol.
Among other important issues noted in this investigation was that the investigator did not wait the 30 days to enroll subjects in the study. An IND does not go into effect upon FDA’s receipt of the IND submission. Rather an IND generally goes into effect 30 days after FDA receives the application, or on earlier notification by FDA that the clinical investigation in the IND may begin (21 CFR 312.40(b)). The FDA emphasized that FDA regulations require a sponsor to submit, and to have in effect, an IND before initiating a clinical investigation that must be conducted under an IND in accordance with 21 CFR 312.40.
For more details about the inspection of this study and the findings of the FDA please review the Warning Letter to Dr. Davd M. Lubeck.
Developing a Mobile Health App?
Updated FTC-HHS online tool helps developers understand which federal laws apply
The Federal Trade Commission (FTC) in conjunction with the Department of Health & Human Services (HHS) Office for Civil Rights (OCR), the HHS Office of the National Coordinator for Health Information Technology (ONC), and the Food and Drug Administration (FDA) have updated the Mobile Health App Interactive Tool. This tool is designed to help developers of health-related mobile apps understand what federal laws and regulations might apply to them. The guidance tool asks developers a series of high-level questions about the nature of their app, including about its function, the data it collects, and the services it provides to users. Based on the developer’s answers to those questions, the guidance tool will point the app developer toward detailed information about certain federal laws that might apply to the app. These include the FTC Act, the FTC’s Health Breach Notification Rule, the Children’s Online Privacy Protection Act (COPPA), the Health Insurance Portability and Accountability Act (HIPAA), the Federal Food, Drug and Cosmetics Act (FD&C Act), and the 21st Century Cures Act and ONC Information Blocking Regulations.
Developers and others seeking more information about how the HIPAA Rules might apply to their health apps should visit OCR’s HIPAA and Health Apps page, which contains information on how HIPAA applies to a range of example health app scenarios and offers key questions to consider in determining when HIPAA’s regulations cover a particular health app.
IRB Forms – Update
The following forms were updated in the IRB website:
- Sample Cover Letter for a Survey Study.docx (09/02/2022)
- Application Checklist for Initial and Continuing Review Full Board.docx (09/02/2022 – New Contact Information for Institutional Biosafety Committee )
- Application Checklist – Single Patient Expanded Access .docx(9/22/2022)
- Request for Exemption Form .doc(09/30/2022)
- Guidance for Completing Continuation Form.docx (10/12/2022)
- Guidance for Preparing a Chart Review Study .docx(10/12/2022)
- HIPAA Authorization to Use and Disclose – Spanish.doc (11/7/2022)
The following forms were added to the IRB website:
- Instructions for Facilitated Review for Collaborative Research with Neighboring Facility .docx(10/12/2022)
The following educational resources were added to the IRB website:
- NIH Policy for Data Management and Sharing (effective 1/25/2023)
- NIH Guide for Writing a Data Management & Sharing Plan
- Data Storage Finder (tool from Cornell University)
National Institute of Health (NIH) Policy for Data Management and Sharing
Investigators Resources
The National Institute of Health (NIH) has posted a one-page handout “The Who, What, Where and When of the NIH Data Management and Sharing (DMS) Policy” summarizing the most important information for investigators regarding the NIH Policy for Data Management and Sharing. Click on the image to go to their website and explore the info/links in the handout.
The University of Pennsylvania has shared the following resources on its website to aid investigators to comply with the National Institute of Health (NIH) Policy for Data Management and Sharing
NIH’s checklist that walks researchers through the elements of a DMSP
NIH is constantly updating its FAQ page on the DMSP. Check back for your questions.
Includes NIH webinar recordings and registration information for upcoming presentations.
Provides points to consider and sample language for informed consent documents of research studies which plan to store and share data and/ or biospecimens for future use.
Penn Libraries uses DMPTool to assist with writing data management plans. DMPTool is a resource researchers can use to draft data management plans. The new NIH DMSP template is available in the tool. We can provide comments on your DMSP if you need assistance. See our contact information on this page.
The National Institute of Mental Health (NIMH) has developed four example DMSPs that are consistent with NIMH and NIH requirements.
NIH institutes and centers may have other data sharing requirements in addition to the NIH DMS Policy. Make sure to read your applicable policy carefully.
A comprehensive listing of all NIH activity codes that generally require applicants to submit a Data Management & Sharing Plan
Provides an overview of ICPSR’s NIH funded archives and recommendations for designating ICPSR for your data to meet the requirements of the NIH DMSP.
Created by librarians and other research support professionals, this working group has created a variety of resources that researchers can use to prepare for the NIH DMS Policy implementation. Resources include glossaries, a DMSP checklist for researchers, and an example DMSP for the 2023 expectations.
Recent article on the NIH DMSP policy that covers 10 key recommendations for creating a DMSP that is both maximally compliant and effective.
Research Data & Digital Scholarship Data Sharing Services
NIH Repositories
Cornell University has excellent resources and tools on its website to aid investigators to comply with the National Institute of Health (NIH) Policy for Data Management and Sharing.
In addition, the NIH National Library of Medicine has posted the following resources:
Office of Human Research Protection (OHRP) Luminaries Lectures Series
Educational Resources for Investigators
The Office of Human Research Protection Luminaries Lectures Series features videos by esteemed individuals with thought-provoking insights on diverse aspects of human research protections.
Some of the recently added videos are listed below. These videos are covering the challenges of research during public health emergencies and research studying usual care practices, as well as thoughts from representatives in the research community on how to promote diversity and engagement in research participation:
- “The Covid Drug Wars” – What We Learned from the Front Lines
- “Unusual Practices Masquerading as Usual Care”
- “Vulnerability, Justice, Equity, and Engagement: A Conversation About Public Health and Human Subjects Research”
Click here and start watching!
Changes in the HSPP/IRB
Administrative Manager and Deputy Director of HSPP: Julia Blair has been named Administrative Manager of the HSPP, after filling the role on an interim basis since June following Deb Gibb’s retirement. She can be reached at jblair@uchc.edu and (860) 679-7555.
HSPP- July, August, September, 2022 – Newsletter
HSPP- July, August, September, 2022 – Newsletter
Revision to Exemption Category 4 (iii)
To ensure the protection of identifiable private information (IPI) at UConn Health in compliance with The Privacy Rule, the HSPP will limit use of the exemption 45 CFR 46.104(d)(4)(iii):
Secondary research uses of identifiable private information, [when] the research involves only information collection and analysis involving the investigator’s use of identifiable health information (not biospecimens) when that use is regulated under [HIPAA].
Exemption 4(iii) applies to secondary research ‘use’ of the IPI which is protected under HIPAA, however the release, transfer or provision of access to a non-covered entity / third party would constitute a ‘disclosure’ where the IPI is no longer protected and the exemption would not apply.
Effective October 1, 2022, to ensure compliance with HIPAA and the Common Rule (45 CFR 46), the UConn Health HSPP will restrict the use of exempt category 4(iii) to studies where the Principal Investigator is UConn Health faculty (whose home/primary institution is UConn Health) and the data is not shared outside UConn Health or with non-UConn Health personnel.
New applications to the IRB seeking approval for secondary research use of identifiable private information which do not qualify for exemption under category 4 should request expedited review by the IRB. More information on exempt and expedited submissions can be found on the HSPP website or by contacting the HSPP Education Specialist, Mayra Cagganello at x8802 or cagganello@uchc.edu.
National Institute of Health (NIH) Policy for Data Management and Sharing
The National Institute of Health (NIH) Data Management and Sharing policy was published on October 29, 2020, and will go into effect on January 25, 2023. The two year delay in implementation was planned to give time to institutions to learn and prepare for enactment of the policy.
This policy applies to all research funded (in whole, or in part) or conducted by NIH that results in generation of scientific data. The goal of this NIH Data Management and Sharing policy is to benefit everyone, namely investigators, funding agencies, the scientific community, and, most importantly, the public. Data sharing provides more effective use of NIH resources by avoiding unnecessary duplication of data collection. It also conserves research funds to support more investigators. As stated in this policy “data sharing enables researchers to rigorously test the validity of research findings, strengthen analyses through combined datasets, re-use hard-to-generate data, and explore new frontiers of discovery.”
The NIH DMS Policy requires researchers to submit a plan to preserve, to share the data and to show compliance with said plan.
The NIH has made available multiple educational materials to inform and educate researchers about this policy at sharing.nih.gov. Below please find the links to the webinars
Webinar I: Understanding the New NIH Data Management and Sharing Policy –
o Resource Slide Deck
o Webinar Recording
Webinar II: Diving Deeper into the New NIH Data Management and Sharing Policy
o Resource Slide Deck
To access the frequently asked questions regarding this policy please click on 2023 Data Management & Sharing Policy
Uconn Health – Research Participant Feedback Form
Now available in Redcap
The Human Subjects Protection Program (HSPP) is responsible for ensuring that studies are conducted in compliance with internal policies, federal regulations and ethical standards. When research participants complete and submit a Research Participant Feedback Form, the HSPP is able to learn about the study volunteer experiences.
Participants can access the Research Participant Feedback form in two ways:
1) Download the form from the IRB website at http://research.uchc.edu/rcs/hspp/volunteers/. Forms must be completed and emailed or faxed following the instructions on the form.
2) *NEW* Research participants may submit this form electronically by accessing the REDCap form at https://redcap.link/UConnHealth-Feedback-Research from a computer or mobile device.
The IRB and HSPP encourage the research community to help research volunteers to complete this form.
IRB Forms – Update
The following updates have been made to IRB forms:
Added new contact information to the following forms:
• Application Checklist for Initial and Continuing Review Full Board.docx (09/02/2022 – New Contact Information for Institutional Biosafety Committee)
• IRB Website : Related Departments and Committees-
Institutional Biosafety Committee (IBC): Investigators must obtain approval from the IBC prior to seeking local IRB approval for research studies that deal with recombinant DNA. Investigators may contact Vijayasmitha Rayadurg in the Office of Research Safety for additional information.
Added new template language to the following form:
• Sample Cover Letter for a Survey Study.docx (09/02/2022)
Changes to the Requests for Exemption form to limit Exempt Category 4 (iii) to researchers and activities internal to UConn Health.
• Request for Exemption Form .doc (09/30/2022)
Continuing Review Guidance
Considerations for When the IRB Evaluates the Progress of a Research Study
According to Robert J. Amdur & Elizabeth A. Bankert. IRB Management and Function. 2nd Edition., Jones & Bartlett, 2006, “Continuing review is a monitoring mechanism that assures that continuing safeguards are in place to protect the rights and welfares of research participants.”
When a Protocol/study is submitted for renewal or continuing review the investigator is to report the study progress and findings. When conducting the continuing review, OHRP recommends that IRBs evaluate the following issues to determine whether the study’s approval should be renewed:
Consistent with the IRB-approved Protocol
The IRB should confirm that the information provided by the investigator at the time of continuing review is consistent with the research protocol previously approved by the IRB.
Total Subject Enrollment
Evaluating information about the number of subjects enrolled in the research at the time of continuing review may allow the IRB to ascertain whether enrollment is consistent with the planned number of subjects described in the IRB-approved protocol. Has accrual progressed as planned? If not, will this affect the ability of the researchers to complete the study?
A marked difference between the actual and expected rates of enrollment may indicate a problem with the research project that requires further evaluation, including whether the research project is likely to provide sufficient data to answer the scientific question(s) being posed.
Subject Withdrawals
Subjects may discontinue their participation in research at any point for various reasons (e.g., serious adverse events, conflicts with the investigators, transportation problems, etc.).
The IRB’s continuing review procedures in general should provide for review of:
• The number of subjects who discontinued their participation; and
• A summary of the reasons for the withdrawals, if known.
IRB review of this information may shed light on problems related to the conduct of the research.
To provide an accurate account of the enrollment data, UCONN Health IRB recommends that prior to completing a Continuation form in the iRIS submission system, the Principal Investigator should have the enrollment information for the study available. If this is not the first request for continuation (e.g. study has been open form more than one year), the enrollment data should build off of the previously submitted request for continuation. Investigators should use the enrollment data in the previously approved continuation form as a starting point. The Enrollment Guidance.docx should be reviewed to provide an accurate account of enrollment numbers, screen failures or withdrawals.
Office of Human Research Protection (OHRP) – Resources
Luminaries Lecture Series
OHRP continues to add new videos to help the research community learn about multiple topics.
Click here to view the latest videos of distinguished speakers from OHRP’s Research Community Forum co-sponsored with Northwell Health this past May.
New additions include:
• The COVID Drug Wars That Pitted Doctor vs. Doctor
• Improving Health Equity in Clinical Research
• Vulnerability, Justice, Equity, and Engagement, A Conversation Public Health and Human Subjects Research
• Unusual Practices Masquerading as Usual Care
HSPP Newsletter – April, May, June, 2022
HSPP Newsletter – April, May, June, 2022
FDA Warning Letter Regarding the Failure to Ensure IRB Continuing Review and Approval of Protocol
Inspections of clinical trials are conducted as a part of the U.S. Food and Drug Administration (FDA)’s Bioresearch Monitoring Program. These inspections are designed to evaluate the conduct of research and to help ensure that the rights, safety, and welfare of human subjects have been protected. Below you will find a short summary of a warning letter issued because of the failure to obtain continuing review of a study and failure to perform study procedures as required by the protocol.
Warning letter to Sabine S. Hazan, M.D.
On February 28, 2022, the FDA issued a warning letter to Dr. Hazan. The FDA officials who inspected the study concluded that the investigator did not adhere to the FDA regulations governing the conduct of clinical investigations and the protection of human subjects. Dr. Hazan failed to obtain continuing review and approval for her study. Specifically, her study IRB approval lapsed. During the course of this lapsed period, she enrolled and randomized subjects into the protocol, and administered investigational drugs to subjects. In addition, she was unable to provide a corrective action plan to prevent the recurrence of this type of violation in the future.
The FDA emphasized that the failure to ensure continuing IRB review and approval, impeded the IRB’s ability to determine the adequacy of the application to conduct the protocol. This raised significant concerns about the extent to which subjects’ rights and welfare were protected at that site during the lapse in approval.
For more details about the inspection of this study and the findings of the FDA please review the Warning Letter – Sabine S. Hazan, M.D. February 28, 2022
Warning letter to Smitha C. Reddy, M.D. / ACRC Studies, LLC
On May 27, 2022, the FDA issued a warning letter to Dr. Reddy. The FDA officials who inspected the study concluded that the study as it was implemented raised significant concerns about the safety of subjects enrolled and the reliability of data at that site.
Dr. Reddy failed to ensure that the investigation was conducted according to the investigational plan. Specifically, the investigator did not ensure subjects randomized to an assigned treatment arm received the correct drug for that group, and there was a failure to adhere to procedures for the blinding of staff.
The FDA emphasized that the principal investigator is ultimately responsible to ensure that the study is conducted properly and in compliance with FDA regulations, both to protect the rights, safety, and welfare of study subjects and to ensure the integrity of study data. Additionally, the FDA required corrective actions to include retraining of the investigator on study drug administration, not just study staff.
For more details about the inspection of this study and the findings of the FDA please review the FDA Warning letter to Smitha C. Reddy, M.D./ACRC Studies, LLC
Office of Human Research Protection (OHRP) – Resources
The Office of Human Research Protection (OHRP) has launched two interactive programs to help explain the expectations for investigators in applying the Common Rule review criteria of equitable selection of subjects in research and minimizing research risks for participants. These resources are valuable for investigators to understand and fulfill these specific requirements for protecting human participants in research.
To access these interactive programs click on links below.
Equitable Selection of Subjects : This is a 30-minute scenario which examines how investigators could apply the concept of equitable selection of subjects in research
Minimizing Risks in Research : This is a 30-minutes scenario which examines the concept of research risks and how these risks to participants could be identified and minimized.
Human Subjects Training – Frequently Asked Questions
I am a new resident/student at UCONN Health and I completed CITI Training under my affiliation with a former institution. Is that CITI Certificate valid at UConn Health?
If an individual is to be included in an IRB application and that person has recently become affiliated to UConn Health (e.g. a new student), that person should attach the CITI Training certificate completed under his/her former affiliation. If the courses previously completed are comparable to the ones required by UCONN Health IRB that individual will not need to complete additional training. If not, he/she must complete training under his/her affiliation to UConn Health. The CITI Program will give credit for any modules he/she have completed under other institution’s affiliation and will require completion of modules that are specific to UConn Health.
To affiliate an account in the CITI Program with UConn Health, individuals should log into the CITI program, and click on “Add Affiliation” listed under the “Courses” Menu. To
find UConn Health in the drop down box, the following words “University of Connecticut“ must be typed. Then, select “University of Connecticut Heath Center”. To complete the process, check the box next to the statement: “I AGREE to the Terms of Service for accessing CITI Program materials” and check the box with the statement: “I affirm that I am an affiliate of University of Connecticut Heath Center.” Last, click on “Continue.”
To select the correct learning group and courses, follow the “Course Enrollment Questions” posted at https://ovpr.uchc.edu/services/rics/hspp/citi-instructions/
Recent Articles Published by a Central IRB
ADVARRA IRB:
What do I do about Incidental Findings in Research? If you are conducting research that has a potential to uncover an incidental finding, it is best to plan ahead for how you’ll treat the result and if you plan to return that result to a participant. This article describes the plans and consideration to communicate incidental findings to research participants.
eClinical Regulatory Trends Impacting Clinical Research For the past two years, the clinical research industry has seen an acceleration in staff shifting to a remote, work from home model. While this was initially in an effort to keep everyone safer from the COVID-19 pandemic, many organizations are permanently moving toward a remote or hybrid work model for their staff. This article discusses how has this shaped current regulatory trends, the benefits of eClinical suite, and the consideration when adopting an eClinical suite.
IRB Forms – Update
Added new contact information to the following forms:
- Human Subject Research Determination Form.doc
- dbGaP Access Request Form for IRB Certification.docx
- Participant Feedback Form.doc
- Participant Feedback Form in Spanish.docx
- HIPPA Assurance of Preparatory to Research or Decedent Research .doc
- Instructions for Students Residents or Fellows Doing Research_at_Hartford HealthCare_or_CT Children’s Medical Center.docx
Added Federal required Overview section to:
Upcoming changes in at the HSPP/IRB and the OVPR
- Vice President for Research: Dr. Pamir Alpay has been appointed Interim Vice President for Research, Innovation & Entrepreneurship while Dr. Radenka Maric is serving as Interim President of the University of Connecticut.
- Associate VPR and Institution Official: Dr. Victor Hesselbrock has been named Interim Associate Vice President for Research Integrity and Regulatory Affairs and Institution Official following Dr. Byerly’s departure.
- Manager and Deputy Director of HSPP: Deb Gibb retired June 1, after 19 years with the HSPP. Julia Blair will serve as interim manager of the HSPP.
HSPP – January, February, March, 2022- Newsletter
HSPP – January, February, March, 2022- Newsletter
How to Write a Low Literacy Informed Consent Form
Obtaining informed consent in non-exempt research is a process required by federal regulations –the U.S Department of Health and Human Services ( HHS) at 45 CFR 46 and the U.S. Food and Drug Administration (FDA) at 21 CFR 50. The consent process typically includes providing a written consent document containing the required information along with an oral presentation of that information to prospective participants. However, for a consent process to empower individuals to voluntarily participate in a study or not, the information in the consent document must be presented in a language they can understand. The readability of a consent form is essential to enable potential participants to have sufficient comprehension of the elements that facilitate a decision. The language used in consent forms should not be complex. An 8th grade reading level is the suggested benchmark to use as the readability index.
Investigators conducting clinical trials should consider literacy of potential participants when preparing consent documents.
John Hopkins Office of Human Subjects Research and Elizabeth Winslow offers the following guidance for preparing consent forms:
- Recommendations to lower the reading level of consent forms:
Words
- Use words familiar to the non-medical reader.
- If possible, keep words to 2- 3 syllables or fewer.
- Use common, familiar words
Sentences/Paragraphs/Print Size & Type:
- Write short, simple, and direct sentences.
- Keep paragraphs short and limited to one idea.
- Use active verbs.
- Use the second person (you) not third person (the participant) to increase personal identification.
- Avoid contractions.
- Use page numbers
- Use at least 12-point font and consider a larger font based on your audience.
- Check the text to see if each idea is clear and logically sequential.
- Avoid large blocks of printed text.
Avoid Complex Medical Terminology
- Avoid medical Terminology. If a medical term must be used, define /explain it
- Be consistent with use of all terminology, such as drug names and abbreviations.
- Use the appropriate abbreviation the first time a drug name is used in the consent.
Abbreviations:
- Spell out abbreviated terms the first time you use them
- Abbreviation terms such as DNA, HIV and AIDS that have come to be accepted as standard by your proposed study population need not be spelled out.
- Do not use e.g. or etc., use instead, “for example,” “so forth.”
- Spell out acronyms when first used.
Pictures
- Use photos, graphics, tables, illustrations or diagrams if they will help clarify procedures.
Numbers
- Use numerals rather than words for numbers, e.g., “10” instead of “ten,” “1 out of 4” instead of “one out of four.”
Tips to Describe Study Procedures
- Consent forms for projects that involve collection of blood or other fluids should include the amount(s) to be taken. Do not use ml. or cc. as a volume measure; give a volume equivalent in teaspoons or tablespoons. Rather than abbreviating such words as teaspoon and tablespoon, please spell them out.
- Do not use symbols such as “>”; use “greater than.”
- Describe study design procedures such as “double blind,” “randomized,” and “placebo/controlled” when the concept(s) is/are first introduced. Example: “A placebo is an inactive substance that looks like the study drug, but contains no medication.”
- Do not use the words “treatment” or “therapy” to describe an investigational drug, device or procedure. Use the term “study drug” not “study medication” when the drug is investigational. The word “medication” or “medicine” should only be used if the drug is commercially available for that particular condition.
- Do not use the term “treatment” or “therapy”” if one of the study arms will be a placebo. Instead, use words like: “study product”, “study drug or placebo”, “study regimen” or “study procedure
- Do not describe investigational drugs, devices or procedures as “new.”For investigational drugs or devices, state they are investigational or “experimental” and describe that term (e.g., the word “investigational” means the study drug is not approved by the U. S. Food and Drug Administration (FDA) and is still being tested in research studies.) Be consistent in using “investigational” throughout the consent form.
- Use “research study,” instead of “trial.”
- Use the word “participant” in the consent form instead of “patient” since this is research. However, you may use “patient” when referring to the person prior to his/her entering the study.
- When describing randomization for 2 groups use, “like the flip of a coin,” for more than 2 groups, use “like drawing numbers from a hat.”
To check the grade level of a consent document, the investigator can implement the following steps.
For Microsoft Word:
- on the “File” tab, click the “Options” button;
- on the “Proofing” tab, under “When correcting spelling and grammar in Word”, make sure “Check grammar with spelling” is selected;
- under “When correcting spelling and grammar in Word”, select the “Show readability statistics” check box. Click on OK
- Click on the “Review Tab”
- Click on “Spelling & Grammar”
After the grammar check is complete, Word displays a message box showing you the readability grade-level.
D- The following websites and word substitution file are helpful for drafting consent forms:
- a) Glossary of medical words: (http://kidshealth.org/kid/word/)
b) Clinical Research Glossary: (http://www.firstclinical.com/icfglossary/)
c) Glossary of lay terms: (http://humansubjects.stanford.edu/general/glossary.html)
- The following Checklist for Low Literacy Informed Consent Forms .pdf has been posted in the UCONN Health IRB website
| Checklist
How to write a Low Literacy Informed Consent Form
|
|
|
Recommendations to lower the reading level of consent forms
|
Check |
| Words | |
| Use words familiar to the non-medical reader | |
| If possible, keep words to 2- 3 syllables or fewer | |
| Use common, familiar words | |
| Sentences/Paragraphs/Print Size & Type | |
| Write short, simple, and direct sentences | |
| Keep paragraphs short and limited to one idea | |
| Use active verbs | |
| Use the second person (you) not third person (the participant) to increase personal identification | |
| Avoid contractions | |
| Use page numbers | |
| Use at least 12-point font and consider a larger font based on your audience | |
| Check the text to see if each idea is clear and logically sequential | |
| Avoid large blocks of printed text | |
| Avoid Complex Medical Terminology | |
| Avoid medical terminology. If a medical term must be used, define/explain it | |
| Be consistent with use of all terminology, such as drug names and abbreviations | |
| Use the appropriate abbreviation the first time a drug name is used in the consent | |
| Abbreviations | |
| Spell out abbreviated terms the first time you use them | |
| Abbreviated terms such as DNA, HIV and AIDS that have come to be accepted as standard by your proposed study population need not be spelled out | |
| Do not use e.g. or etc., use instead, “for example,” “so forth.” | |
| Spell out acronyms when first used | |
| Pictures | |
| Use photos, graphics, tables, illustrations or diagrams if they will help clarify procedures | |
| Numbers | |
| Use numerals rather than words for numbers, e.g., “10” instead of “ten,” “1 out of 4” instead of “one out of four.” | |
|
Tips to Describe Study Procedures
|
|
| Consent forms for projects that involve collection of blood or other fluids should include the amount(s) to be taken. Do not use ml. or cc. as a volume measure; give a volume equivalent in teaspoons or tablespoons. Rather than abbreviating such words as teaspoon and tablespoon, please spell them out. | |
| Checklist
How to write a Low Literacy Informed Consent Form
|
|
|
Tips to Describe Study Procedures
|
Check |
| Do not use symbols such as “>”; use “greater than.” | |
| Describe study design procedures such as “double blind,” “randomized,” and “placebo/controlled” when the concept(s) is/are first introduced. Example: “A placebo is an inactive substance that looks like the study drug, but contains no medication.” | |
| Do not use the words “treatment” or “therapy” to describe an investigational drug, device or procedure. Use the term “study drug” not “study medication” when the drug is investigational. The word “medication” or “medicine” should only be used if the drug is commercially available for that particular condition | |
| Do not use the term “treatment” or “therapy”” if one of the study arms will be a placebo. Instead, use words like: “study product”, “study drug or placebo” | |
| Do not describe investigational drugs, devices or procedures as “new.” For investigational drugs or devices, state they are investigational or “experimental” and describe that term (e.g., the word “investigational” means the study drug is not approved by the U. S. Food and Drug Administration (FDA) and is still being tested in research studies.) Be consistent in using “investigational” throughout the consent form. | |
| Use “research study,” instead of “trial.” | |
| Use the word “participant” in the consent form instead of “patient” since this is research. However, you may use “patient” when referring to the person prior to his/her entering the study. | |
| When describing randomization for 2 groups use, “like the flip of a coin,” for more than 2 groups, use “like drawing numbers from a hat.” | |
|
To check the grade level of a consent document, the investigator can implement the following steps
|
|
| For Microsoft Word:
1. on the “File” tab, click the “Options” button; 2. on the “Proofing” tab, under “When correcting spelling and grammar in Word”, make sure “Check grammar with spelling” is selected; 3. under “When correcting spelling and grammar in Word”, select the “Show readability statistics” check box. Click on OK 4. Click on the “Review Tab” 5. Click on “Spelling & Grammar” After the grammar check is complete, Word displays a message box showing you the readability grade-level. |
|
ResearchMatch, an Online Recruitment Tool
ResearchMatch.org is a national online recruitment tool for health research, funded by the National Institutes of Health and maintained at Vanderbilt University. ResearchMatch connects health researchers with individuals interested in volunteering through its secure online matching tool, available in English and Spanish. UConn Health is part of the ResearchMatch Network and there is no cost to UConn Health researchers to use ResearchMatch. There are currently over 160,000 (and counting!) registered volunteers across the country.
To see if ResearchMatch might be useful to you, register now to conduct a feasibility analysis:
Register here: https://www.researchmatch.org/researchers/. (You do not need to be a Principal Investigator to register.) The registration process takes less than 10 minutes. Registration grants you “feasibility access” to search the current ResearchMatch volunteer population for demographic and health information of volunteers within a designated geographic area.
Then, if you decide to use ResearchMatch to conduct participant recruitment, you will need IRB approval. Once approved, you may request “recruitment access” in ResearchMatch and upload your IRB approval letter and your IRB-approved contact message. Recruitment access will give you the ability to send your contact message to volunteers that you select. If a volunteer agrees, you will be given access to his/her contact information in order to contact about possible study participation.
The next ResearchMatch Training is April 14, 2022 at 3:00 pm.
For questions about how to use ResearchMatch for your health research, please contact ResearchMatch Liaison, Ellen Ciesielski eciesielski@uchc.edu or visit https://ovpr.uchc.edu/services/rics/hspp/resources/researchmatch/.
Office of Human Research Protection (OHRP) – Resources
- OHRP New Informational Resource Flyer with its Very Own QR Code!
OHRP’s new Informational Resource Flyer includes a QR code allowing anyone with a smart phone access to a free online library of trusted resources about research and research participation. Print, display, and distribute this flyer at your centers for the benefit of prospective research participants!
Find the flyer here together with other informational materials (in English and Spanish) that you may wish to print and provide for potential research participants! These resources are free and you do not need permission to distribute them.
- New Interactive Training Programs on IRB Reviews!
OHRP launched two interactive training programs on considerations for reviewing and designing research involving human participants.
OHRP created these programs to enable investigators and IRB reviewers to be cognizant of the importance of diversity, inclusion, and risk minimization in research participation.
Click here to access our other scenarios!
- Recordings of OHRP Presentations on Human Subjects Research and Investigator Responsibilities for Protecting Participants in Research!
What is Human Subjects Research? A Review of the Common Rule and its Application provides helpful explanation on the complex concept of human subjects research and how to address related considerations in the NIH grant application process.
What Investigators Need to Know About IRB Review helps investigators understand the thoughts and considerations needed for writing a successful plan to protect human research participants that would pass the muster of reviewers.
These videos will help investigators with the NIH grant application and IRB review process.
HSPP- OCTOBER -NOVEMBER-DECEMBER, 2021- NEWSLETTER
HSPP- October-November-December, 2021- Newsletter
FDA Warning Letter Regarding the Failure to Submit INDs for the Conduct of Clinical Investigations with an Investigational New Drug
Inspections of clinical trials are conducted as a part of the U.S. Food and Drug Administration (FDA)’s Bioresearch Monitoring Program. These inspections are designed to evaluate the conduct of research and to help ensure that the rights, safety, and welfare of human subjects have been protected. Below you will find a short summary of warning letters issued because of the failure to submit investigational new drug applications.
Warning letter to Kaleido Biosciences, Inc
On September 7, 2021, the FDA issued a warning letter to Kaleido Biosciences, Inc. The FDA officials inspected two of Kaleido’s studies and concluded that investigators did not adhere to the FDA regulations governing the conduct of clinical investigations and the protection of human subjects.
Kaleido investigators thought that the product used in their investigations was subject to regulations as medical food but not subject to regulations as a drug. However, the FDA inspectors concluded that the product was intended for use as a drug, and not as a food.
The argument established by the FDA to support their conclusion is based in the definition of food vs a drug in the use of a clinical investigation. The FDA argued that the purposes of this clinical investigation was to evaluate the efficacy of a food product as treatment of a disease and, consequently, the food in this trial was seen as a drug. Therefore, use of the food product in the clinical trial is not exempt from the investigation new drug requirements.
For more details about the inspection of these studies and the findings of the FDA please review the warning letter to Kaleido Biosciences, Inc.
Warning letters to Jon B. Cole, MD, and Lauren R. Klein, MD., MS.
The FDA regulations require a sponsor to submit, and to have in effect, an investigational new drug application (IND) before initiating a clinical investigation of a drug in human subjects, unless the clinical investigation qualifies for an exemption (see 21 CFR 312.20 and 312.40(a)).
The FDA determined that Dr. Cole and Dr. Klein failed to comply with these requirements while using marketed drugs in two studies.
The investigators thought that an IND was not needed, and argued that the medications administered to subjects were not part of a research intervention but were provided only for clinical purposes. In addition, the investigators stated that if their clinical investigations were subject to FDA jurisdiction, they met the criteria for exemption from the investigational new drug requirements.
Contrary to the investigators, the FDA auditors concluded that the studies were designed to study the safety and efficacy of those marketed drugs products. In addition, the FDA determined the drugs were not delivered in the course of medical practice, but for research purposes. “The FDA underlined that whenever an investigator limits his choices, his patients’ choices, and the choices of the people working for them in the treatment of patients, then he/she is conducting a clinical investigation. This is different from the practice of medicine, where the primary intent is to treat the individual patient.”
Moreover, the FDA inspectors determined these clinical investigations did not meet the criteria for exempt since these investigations increased the risks or decreased the acceptability of the risks associated with the use of the drug products.
For more details about the studies mentioned above, the FDA’s thinking regarding IND requirements for market drugs and FDA views of clinical use vs. clinical investigation, please click on the links to the warning letters seen below:
Medical Devices
Medical device products are regulated by the FDA’s Center for Medical Devices and Radiological Health (CDRH). Depending on the device classification and other factors, the Code of Federal Regulations, Title 21, defines the requirements to approve or clear devices sold in the United States.
Investigators planning to conduct research with medical devices should learn the FDA status of a device. The investigator should determine whether the device has been approved, cleared for marketing, or whether it is an investigational device. When used in research it is important that the informed consent form accurately identify the type of device being used as approved, cleared, or investigational (see FDA guidance).
Reviewing the following information will allow investigators to understand the process by which the FDA classifies devices, clears devices, and approves devices. The sections below includes excerpts from the document titled Is it really FDA approved? and the FDA webpage on the Premarket Notification 510(k) clearance process.
Overview of Device Regulation
FDA classifies devices, or more accurately device types, in order to identify the degree of regulations for that product area. Classification is based on two factors: the device description/its physical characteristics, and the intended use.
FDA classifies devices into Class I, II, or III. The class of the device generally increases with its degree of risk. Regulatory control increases from Class I to Class III. The device classification regulation defines the regulatory requirements for a general device type. Most Class I devices are exempt from Premarket Notification 510(k); most Class II devices require Premarket Notification 510(k); and most Class III devices require Premarket Approval.
A description of device classification and a link to the Product Classification Database is available at “Classification of Medical Devices.” To learn more about how medical devices are classified, please watch the FDA educational video titled: How is my Medical Device Classified?
Note – A registration number with the FDA only means the FDA is aware of the manufacturer and device, and does not mean the device is ‘FDA cleared’ or ‘approved.’ (see more info here)
Cleared Devices
The FDA may clear a device for marketing through the 510(k) process, when the manufacturer demonstrates the device is substantially equivalent to a predicate device. A claim of substantial equivalence does not mean the device(s) must be identical. Substantial equivalence is established with respect to intended use, design, energy used or delivered, materials, performance, safety, effectiveness, labeling, biocompatibility, standards, and other applicable characteristics. The 510K clearance process does not require submission of clinical data to support the claim.
A device which is “cleared” to market should not be deemed the same as a device that has been “approved” by the FDA through a Premarket Approval (PMA) application.
Approved Devices
To receive FDA approval to market devices, manufacturers must demonstrate with sufficient, valid scientific evidence (i.e., submitting clinical data to support a claim) that there is a reasonable assurance that the devices are safe and effective for their intended use.
Investigational Devices
An investigational medical device is one that is the subject of a clinical study designed to evaluate the effectiveness and/or safety of the device. An application for an Investigational Device Exemption (IDE) is to be submitted by the Sponsor or investigator to use the investigational device/unapproved device in a clinical study.
Data collected during these clinical studies is to be included in a future marketing application. The IDE application enables manufacturers to ship a device from one state to another when conducting a clinical study on the device without being subject to most other provisions of the Federal Food, Drug, and Cosmetic Act.
An IDE application may also be required for a legally marketed device that has been modified and/or intended for a new use.
Clinical studies with investigational devices of significant risk must be approved by FDA and by an Institutional Review Board (IRB) before the study can begin. Studies with devices of no significant risk must be approved by the IRB only before the study can begin.
Investigators conducting research with medical devices are to include in their initial application and informed consent forms whether their devices are approved devices, cleared devices or investigational devices.
Inclusion of Certificate of Confidentiality Language in Consent Forms for NIH funded Studies
In October 2017, NIH updated its Policy for issuing Certificates of Confidentiality (Certificates or CoCs) for NIH-funded and conducted research. These Certificates protect the privacy of participants by limiting the disclosure of identifiable, sensitive information.
Informed consent forms of NIH funded studies must include the required language regarding the Certificate of Confidentiality (CoC) and the protections it offers. This requirement is already listed in the Main Consent Form Template .doc (page 8) and the Main Consent Form Checklist.doc (Page 4)
More information about Certificates of Confidentiality is available at https://grants.nih.gov/policy/humansubjects/coc.htm
IRB Forms – Update
The submission checklists for IRB applications have been updated.
The updates include:
- Changing the point of contact for I.T. security
- Clarifying details regarding the need for letters of permission to conduct research
- Clarifying details regarding the FERPA verification form
- Clarifying details regarding the use of recruitment tag lines for on-line postings
HSPP- July-August-September, 2021- Newsletter
HSPP- July-August-September, 2021- Newsletter
Informed Consent- Process & Documentation
The informed consent process is one of the central components of the ethical conduct of non-exempt research with human subjects. The consent process typically includes providing a written consent document containing the required information along with an oral presentation of that information to prospective participants. The informed consent process involves the “who”, “what”, “when’, “where”, and “how” that results in a valid, and effective informed consent being obtained from a participant.
The following section presents a general overview of an effective informed consent process and its documentation. Exceptions to this process may be granted by the IRB. Those exceptions are described in IRB policy 2011-008.2.pdf – Informed Consent – Waivers and Alterations.
Who can obtain consent?
The Principal investigator or designated individuals listed on the materials approved by the IRB. Any personnel authorized to obtain consent must comply with human subjects protection training requirements. Individuals who are approved to obtain consent must be knowledgeable of the protocol and prepared to answer questions that may be posed by the potential subjects.
Study personnel who will be obtaining consent should be familiar with the following IRB policies:
- 2011-008.0.pdf– Informed Consent – Forms
- 2011-008.1.pdf – Informed Consent – Process
- 2011-008.5.pdf – Informed Consent – Providing and Obtaining Informed Consent
Who can provide consent?
Consent is to be obtained from an individual who has authority to give consent. If the prospective participant is an adult who has capacity to consent, it is that individual who should give consent. When an individual is unable to consent on his or her own behalf, consent must be obtained from a person who has the authority to do so. Investigators should be aware of the provisions described in the IRB Policy 2011-008.5.pdf regarding the conditions and requirements to obtain consent from adults, minors, and legally authorized representatives.
The study protocol and initial study application should identify who will be providing consent (i.e., adult subjects, legally authorized representative (LAR)). If the individual to provide consent is a LAR, documentation of this status must be obtained except when the LAR is the parent of a participant who has not yet reached the age of majority, or attests to being the next of kin. One exception to the next of kin provision is that adults with intellectual disabilities who have been declared incompetent must have an appointed legal guardian provide consent to participate in research. The natural parents of the adult are not authorized to give permission unless they have been appointed legal guardian(s).
When Consent Process must occur?
An informed consent process must be conducted with a potential subject prior to any involvement of the subject in non-exempt research (e.g., prior to any procedures that are done solely for research purposes). It must happen before any interaction/interventions to collect data to ensure that the subject has an appreciation for the study in which s/he may enroll.
The process of consent should continue throughout the study, for example by explaining each visit as it occurs and ensuring the subject is still willing to participate, or by providing new information to subjects as it is learned to ensure they are still willing to participate.
Where Consent Process must occur?
The consent process must be conducted in a setting that affords sufficient privacy to the potential subject. Privacy refers to an individual’s desire to control who has access to him/herself. The setting where the potential participants will interact with the researcher team must be protected from access to the public.
What do you need to obtain Consent from a prospective participant?
The individual obtaining consent must present the subject with a written informed consent form that contains the key information that is most likely to assist a subject in understanding the research, what is expected of them, and the potential risks of harm and potential benefits, if any. The consent form must be written in a language that is understandable to the subject or subject’s LAR, and should be written in lay language using an 8th grade literacy level as a benchmark. The informed consent template and informed consent checklists available on the IRB website should be used to ensure the consent document contains the regulatory and local required elements of consent.
The individual obtaining consent should ensure that the most recently approved and stamped version of the consent form is used when obtaining consent.
How should a consent process be conducted?
The Principal investigator must describe the proposed process of consent in the material provided to the IRB.
This process should begin with allowing the potential subject time to review the consent document, and then a discussion of the key elements of a research study in the subject-preferred language.
The process must be free of any coercion (e.g. a threat of something bad happening if the subject declines participation), and free of undue influence (e.g. a sense of pressure to say yes, because the person obtaining consent is also the clinical provider). The subject must receive the following information:
- that consent is being sought for research and participation is voluntary;
- the purpose of research;
- expected duration of participation and procedures to be followed;
- the risks or discomforts and the potential for benefits to the prospective subject or to others; and
- the appropriate alternatives procedures or courses of treatment, if any, that might be advantageous to the prospective subject.
The consenter should provide ample time for questions, and may ask the subject questions about the research to assess his/her understanding of the study.
In most cases, unless the IRB has waived the requirement to document consent, at the conclusion of the consent process and after the subject has decided to participate, investigators are to obtain a signature and date of signature from the participant on an IRB approved informed consent document. The IRB also require that the person obtaining consent sign and date the form. At this time, a copy of the signed and dated consent form must be provided to the subject along with the Research Participant Feedback Form
The original signed consent form must be stored in accordance with the plans for storage described in the study application and protocol (e.g., consent form is to be filed in a research folder, or in separate secure location apart from research record, or in the medical record).
Notes in a research chart indicating on-going discussions with the subject at subsequent study visits may supplement documentation of the informed consent process.
Educational Resources for Investigators at UConn Health – Informed Consent Process and Documentation
Checklist and Weekly WebEx Sessions
Investigators may use this Self-Audit /Checklist tool along with the IRB Policies listed above to ensure the consent process and its documentation comply with UConn Health IRB Policies.
| SELF -AUDIT TOOL/CHECKLIST | |
|
INFORMED CONSENT PROCESS & DOCUMENTATION |
Consenter Initials |
| The consent process was conducted using the latest approved and stamped consent form | |
| The consent process occurred in a private setting | |
| The consent process was conducted in a language understandable to the subject | |
| The consent process started with a potential participant being given the opportunity to review the informed consent form and it was followed by a discussion about the research | |
| The process was free of coercion or undue influence | |
| The process provided the subject, sufficient time to discuss, ask questions and consider whether or not to participate | |
| Once the subject had all his/her questions answered and had ample time to consider the information s/he decided whether or not to participate. | |
| If documentation of consent was not waived by the IRB (e.g., informed consent form contains signature lines) informed consent process was documented in an IRB approved informed consent form. | |
| The consent form was signed and dated by the subject (or legally authorized representative) in the section assigned to the participant | |
| The consent form was signed and dated by the investigator in the section assigned to the investigator | |
| All names, signatures and dates were entered in the document on the same date and at the same time | |
| After the signatures were entered in the consent form the participant was provided with a copy of the complete signed informed consent document | |
| At the conclusion of the consent process, the investigator provided a Research Participant Feedback form to the subjects. | |
| The signed consent form has been stored in accordance with the plans for storage described in the study application and protocol (e.g., consent form was filed in research folder, or in separate secure location apart from research record, or in the medical record). | |
The HSPP is offering a one-hour WebEx “Informed Consent Process and Documentation” education session every Thursday and Friday at noon time for study coordinators, investigators, first time principal investigator, and students who plan to conduct Human Subjects Research at UConn Health. To register for these sessions please email Mayra Cagganello at cagganello@uchc.edu
Educational Resources for Investigators –OHRP –Simplifying Informed Consent Video
The Office of Human Research Protection (OHRP) has posted a video titled: “Simplifying Informed Consent.” In this video OHRP representatives discuss what goes into a meaningful informed consent. Practical examples are used to illustrate how to discern meaningful information for potential participants, and how to present information simply in consent documents and materials to ensure consent processes fulfill their goal of enabling potential participants to make informed decisions about whether to participate in the research.
To access this Simplifying Informed Consent video please click here
Informed Consent – Process & Documentation – Frequently Asked Questions
Why do I need to use the Main Consent Form Checklist to create my Consent Form?
UConn Health IRB created and posted the Main Consent Form Checklist .doc to assist investigators and research staff when creating consent documents. This checklist outlines the basic and additional elements of a consent form.
Although, not all elements of the informed consent form template will be required for every study, as applicable to a study, the IRB recommends inclusion of all relevant elements noted on this form and reserves the right to require additional elements.
In addition, as applicable to the study design, investigators must use additional consent checklists along with the above one when creating their Consent forms. For example, if the study involves genetic research the investigator must also complete the Consent Checklist – Genetic Research Addendum If the research involves the use of stem cells the Consent Checklist – Stem Cell Research Addendum.doc must also be used. When funding for a study comes from the National Institute of Justice, the Consent Checklist – National Institute of Justice Requirements Addendum.doc. must be used along with the main consent checklist.
Do I need to use the Consent Form Template?
UConn Health IRB created and posted the Main Consent Form Template .doc to assist investigators and research staff when creating consent documents. The IRB strongly recommends investigators to use the standard UConn Health Main Consent Form Template .doc because this template contains all the basic elements, and is tailored to multiple study designs (e.g., consent for federal funded research, consent for genetic research, consent for research subject to FDA oversight). However, this template may not cover all nuances for various studies. You may need to add, delete and/or edit sections to make them applicable to your study.
What should I do if I realized I have not documented the consent process correctly (e.g., the subject did not incorporate the date when signing the Informed Consent Form)?
In the event that an informed consent (IC) form is found to be undated, if the error is not discovered while the subject is present, the research staff should prepare a note to file attesting to the fact that they witnessed the signing of the form, and the date that it was witnessed.
Since this incident was under the control of the study team, this event should be reported to the IRB within 5 days of becoming aware of the non-compliance. The investigator should complete and submit a problem report form via iRIS system.
To avoid this type of issues, investigators obtaining consent should review the IC forms once they are signed/completed, and before the subject leaves that day to ensure that all signatures and dates are properly entered on the forms.
Who may provide consent when a subject is unable to provide consent?
When a potential subject is unable to provide consent because of impaired competency, consent must be obtained from a legally authorized representative (LAR) of the subject. Documentation of this status must be obtained except when the LAR is the parent of a participant who has not yet reached the age of majority, or attests to being the next of kin. One exception to the next of kin provision is that adults with intellectual disabilities who have been declared incompetent must have an appointed legal guardian provide consent to participate in research. The natural parents of the adult are not authorized to give permission unless they have been appointed legal guardian(s).
The investigator obtaining consent from a LAR must be knowledgeable of the IRB Policy 2011-008.5.pdf – “Informed Consent – Providing and Obtaining Informed Consent” which describe in detail who in Connecticut meet the definition of a legally authorized representative.
How far in advance of research participation, can informed consent be obtained?
The U.S. Department of Health & Human Services (HHS) do not identify how far in advance of study entry a subject can provide consent. They explain that the amount of time required by a subject to make a decision would presumably depend on the nature of the study, taking into account, among other factors, the degree of risk, potential benefits, alternatives, and desire to consult with family members or others. HHS recommends reviewing the information contained in the consent form with the subject again if a prolonged period elapses from the date of consent to the date of entry into the study.
FDA Regulated Studies -Compliance with 21 CFR Part 11
Title 21 CFR Part 11 is the portion of the Code of Federal Regulations that provides standards determined by the Food and Drug Administration (FDA) on electronic records and electronic signatures. During the COVID-19 pandemic, an FDA enforcement discretion of Part 11 was implemented, which is still in effect. However, this enforcement discretion will eventually end.
If any FDA regulated studies at UConn Health are using work-around solutions from the FDA Guidance on Conduct of Clinical Trials of Medical Products During the COVID-19 Public Health Emergency these systems will need to be discontinued when the Public Health Emergency is declared over.
FDA Sends Warning Letter to Individual Investigator for Clinicaltrials.gov Non-Compliance
For the first time, the FDA sent a warning letter to a principal investigator for a ClinicalTrials.gov record that was not updated in accordance with the law. Civil money penalties currently stand at $12,316 per day until the violation is corrected. Previous warning letters were sent to industry sponsors, but this is the first time the FDA has sent a letter to an individual investigator for non-compliance.
For any questions related to ClinicalTrials.gov, please contact UConn Health’s ClinicalTrials.gov Administrator, Ellen Ciesielski (eciesielski@uchc.edu) for assistance.
HSPP- April-May-June, 2021- Newsletter
HSPP- April-May-June, 2021- Newsletter
What is Exempt Human Subjects Research?
Exempt human subject research is a project that does constitute human subjects research but is exempt/excused from satisfying the requirements of the Department of Health and Human Services (HHS) policy for the protection of human research. Research activities that involves no more than minimal risk are exempt from the human research protection regulations when the only involvement of human subjects falls within one or more of the exempt categories described in the Request for Exemption Form .doc. While the research may be exempt from certain regulatory requirements, human subject protections, such as plans for protection of privacy and confidentiality of data, are still applied per accreditation standards and internal policies.
As per UConn Health’s Human Subjects Protection Program Policy 2011-009.2.pdf – Institutional Review Board – Exemptions, investigators cannot make the determination as to whether a human research project meets the criteria of exempt research. This determination is to be made by the Institutional Review Board (IRB).
To aid those who need to decide if an activity is research involving human subjects that must be reviewed by the IRB for Exempt determination, the Office of Human Research Protection (OHRP) published graphic charts titled Is the Research Involving Human Subjects Eligible for Exemption Under 45 CFR 46.104(d)? .
What is Non-Exempt Human Subjects Research?
If the project does not fall within one or more of the defined categories of exemption, then it is not exempt and must satisfy the regulatory criteria for approval. Non-Exempt human subject research may be a project for which research activities involve no more than minimal risk to subjects and all of the procedures in the research are described in the categories of research that may be reviewed by the expedited procedure. The expedited review procedure means that only one member of the IRB needs to conduct the review. This type of research is reviewed on a daily basis and there are no submission deadlines.
Non-Exempt human subject research may also be a research project involving greater than minimal risk and/or involving procedures not described in the categories for exempt status or expedited review. This type of research would have to be reviewed by the convened IRB committee and submission deadlines will apply.
In order to obtain IRB review investigators must complete and submit an on-line Application in the iRIS submission system and attach to that application the relevant submission checklist and corresponding documents.
IRB Frequently Asked Questions
Q: Who is consider “Key Study Personnel” in a Human Subjects Research Study?
A: The key study personnel (KSP) are those people designated by the Principal investigator as back–up principal investigator, co-investigators, study coordinators, data managers, or consenters on an application submitted to the IRB for review and approval. The KSP often include individuals involved in the study through an interaction or intervention with research subjects for research purposes or those reviewing or accessing identifiable data for the research. Individuals who will be interacting with research subjects during the course of a study, but only in their regular non-research employment capacity (e.g. a nurse or phlebotomist) should not be listed as KSP if they are not associated with the study as researchers.
Q: Do key study personnel added to a study need to complete Human Subjects Training?
A: Yes. All key study personnel listed on an IRB application must complete training in the protection of human subjects. Training completed through the Collaborative IRB Training Initiative (CITI) is the most used method of training to fulfill this requirement. Training must have been completed within the past three years to be considered current.
Q: I have little experience in IRB submissions. Where can I find information about the IRB process for a new proposed study?
A: The Human Subjects Protection Program offers a one-hour general educational session for study coordinators and investigators who plan to conduct Human Subjects Research at UConn Health. This training provides an overview of the research proposal submission and maintenance process. Registration is required. Interested staff should e-mail Mayra Cagganello at cagganello@uchc.edu. Individuals who need study specific guidance on preparing IRB submissions are encouraged to request assistance from the Education Specialist as noted above. WebEx orientation sessions are available on a daily basis.
Recent Articles Published by a Central IRB
ADVARRA IRB:
FDA Inspections of Clinical Investigators: Understanding the Process and What to Expect: This article provides answers to a series of questions regarding FDA inspections process.
Among the questions answered in this article are:
- What is the likelihood an investigator-initiated Investigational New Drug application (IND) and non-IND study would undergo an FDA inspection at an academic center?
- For multisite studies, does FDA inspect all sites, or might one specific site be selected to be monitored?
- How do you suggest research staff/coordinators educate clinical investigators (CIs) that they need to pay attention to study oversight and the FDA will not hold coordinators responsible by FDA if things go awry in the study conduct?
- Do you anticipate inspections to pick back up as more people become vaccinated and COVID-19 cases decrease? Will the FDA catch up on missed investigations?
Cell and Gene Therapy vs Small Molecule Research: Understanding the Difference Cell and gene therapy’s popularity has grown exponentially in the past year. This article provides an overview of how cell and gene therapy research is different from traditional drug development. Among the issues discussed in this article is that sites need to build the required infrastructure for conducting cell and gene therapy research safely and successfully.
Educational Resources for Investigators
OHRP Luminaries Lecture Series
The Office of Human Research Protection (OHRP) has posted a series of lectures on human subjects research protections titled: “Luminaries Lecture Series.” Many of these lectures are recordings of keynote addresses at OHRP-sponsored Research Community Forum (RCF) events. Among the topics presented in these lectures are “Use of eConsent in Human Subjects Research,” “Making Mobile Clinical Trials a Reality” and “Big Data, Privacy, and the Public Good.” To access these Luminaries Lecture Series please click here.
HSPP-Newsletter January-February-March 2021
HSPP-Newsletter January-February-March 2021
NIH Releases New Policy for Data Management and Sharing
On October 29, 2020, the National Institute of Health (NIH) published the final policy for data management and sharing (DMS). This policy applies to all research funded or conducted by NIH that results in generation of scientific data. As stated in this policy “data sharing enables researchers to rigorously test the validity of research findings, strengthen analyses through combined datasets, re-use hard-to-generate data, and explore new frontiers of discovery.” The NIH DMS Policy requires researchers to submit a plan to preserve, to share the data and to show compliance with said plan.
To learn more about the scope of this policy and the details of data management and sharing plans, please review the Final NIH Policy for Data Management and Sharing.
Limited Data Sets and Data Use Agreements
A limited data set (LDS) contains protected health information that is associated with indirect identifiers as defined in the HIPAA privacy rule. The indirect identifiers that may be included in an LDS are: town, city, state and five digit or more zip code, dates directly related to an individual such as date of birth, admission date, discharge date and date of death.
Before an LDS can be received by a UConn Health employee or disclosed to another institution, a data use agreement (DUA) must be in place between the sender and receiver of the LDS. This DUA is required under the HIPAA Privacy Rule. This agreement establishes the ways in which the information in the limited data set may be used, the purpose for which it was disclosed, and identifies who is permitted to use or receive the information.
Moreover, the DUA stipulates that the recipient will use appropriate safeguards to maintain the confidentiality and protect the data from further disclosures.
Since the data use agreements establish institutional obligations and bind the institution to the terms of the agreement, investigators are not authorized to execute research DUAs. UConn Health DUAs for research related activities are processed through the Office of Sponsored Programs Sponsored Program Services (SPS) or the Office of Clinical and Translational Research (OCTR). The specific contacts in these offices are listed below:
- If the DUA is related to a Clinical Trial contact: Cherron Payne chpayne@uchc.edu
- If the DUA is unrelated to a Clinical Trial contact: Jennifer Pomales pomales@uchc.edu
IRB Forms – Update
The Main Consent Form Template .doc has been revised to include instructional text about the option to decline payment for participation. The Main Consent Form Checklist .doc has also been revised to reflect this option.
Which Initial Application Form is the Correct One for Your Study?
Once an investigator has determined that his/her project is a human subject’s research project, the next step for the investigator is to submit the project for review and approval to the IRB. This task will require that the investigator complete the “Initial Study Application Form” within the Integrated Research Information System (iRIS).
The investigator creating a new study application in iRIS will need to select one of the three available Initial Study Application Forms listed below:
- Application for a General Study
- Application for a Humanitarian Use Device
- Application for a Registry and /or a Repository
The following section provides a description of the three Initial Application Forms available in iRIS along with examples of when each one should be selected.
Application for a Humanitarian Use Device (HUD):
According to the U.S. Drug and Food Administration (FDA) a Humanitarian Use Device (HUD) is defined as a medical device intended to benefit patients in the treatment or diagnosis of a disease or condition that affects or is manifested in not more than 8,000 individuals in the United States per year. An HUD is an FDA approved device. Because the HUD device is approved for use in such a small population, the FDA regulations requires that an IRB approve the use of the HUD in accordance with its approved label even though the use of the HUD is not research.
If you are requesting approval for use of an HUD, select the application specific for HUDs.
Application for a Registry and /or a Repository:
A registry/repository is used for the collection and maintenance of information/biospecimens on individuals who have a similar condition and who will consent to being contacted for future studies. The investigator must develop a protocol that describes how the data/biospecimens will be collected, how they will be maintained, and how release of information from the registry or biospecimens from the repository will occur.
If you are requesting approval for a Registry and /or a Repository, select the application specific for Registry/Repository.
Application for a General Study:
The Application for a General Study form is the most commonly used application type. The investigators should select it when their research is categorized as either biomedical research, social & behavioral research or community based participatory research. These projects may qualify for Exempt Status or Expedited review in accordance with regulatory criteria, or otherwise they will be review by the convened board.
Examples of human subject research projects that should be submitted with this General Application Form are:
- Minimal risk studies (e.g. studies limited to a survey, studies limited to a retrospective or prospective data review, clinical studies of drugs and medical devices when the conditions for expedited review are met, studies on individual or group characteristics or behavior including, but not limited to, research on perception, cognition, motivation, identity, language, communication, cultural beliefs or practices, and social behavior).
- Studies submitted for full board review (e.g., investigational new drug (IND) studies, investigator new device (IND) studies, social & behavioral studies including more than minimal risk to subjects).
Research with Children
When children are to be involved in non-exempt research, the investigator must address the additional protections for the inclusion of children in research. The investigator does this by completing IRB Form D – Additional Protections for Children Involved as Subjects in Research. The additional requirements set forth on this form are derived from DHHS and FDA regulations.
On Form D the investigator makes the initial assessment of risk level and sets forth plans for obtaining parental permission and assent. The IRB reviews this form and makes the final determination as to whether the requirements for additional protections have been satisfied. Depending on the level of risk of the study, UConn Health IRB will determine whether one or both parents (or legally authorized representatives) must give their permission. The IRB will also make the final determination as to whether assent of the child is required and if so how that assent will be obtained. In making this determination the IRB will take into consideration the age and maturity of the children, and the psychological state of the children involved.
Per UConn Health policy, 2011-006.3.pdf – Additional Protections – Children the additional protections for children apply to all non-exempt research (e.g., Expedited and Full Board Submissions) that is federally funded or supported, and/or that involves an intervention or interaction with a child regardless of funding source. Therefore, the additional protections do not apply to non-federally funded or supported chart review studies that qualify for exempt status.
OHRP New Video
Research with Children: What Parents Need to Know
The Office of Human Research Protection (OHRP) has posted a new video on its public outreach website. This short video titled “Research with Children: What Parents Need to Know” is for parents/legal authorized representatives who may be or have been approach about permitting their children to participate in research. It provides an explanation as to why research-involving children is necessary, its importance and what parents should expect if considering enrolling their child in a study. This video is found under the category of Videos on Protecting Human Research Volunteer
HSPP- October, November, December, 2020- Newsletter
HSPP- October, November, December, 2020- Newsletter
Accessing and Signing-off Submissions in iRIS
In order for a member of the study team to be notified that there is an IRB submission that requires the study team member’s sign-off, there must be a valid e-mail address associated with the study member’s account in iRIS. Therefore, it is important to verify the validity of email addresses when selecting the members of a study team. For UConn Health faculty, staff, students and residents, iRIS is linked to the LDAP active directory at UConn Health; so if a user does not have an e-mail in that directory there will likely be problems notifying them of the required sign-off task in iRIS. In addition to verifying addresses by using the active directory; at the time of adding study team members to the form in iRIS there should be an email address listed next to the team member’s name in iRIS. Lack of a valid e-mail address prevents the submission from being routed to the study team member for sign-off and from being submitted to the IRB for review and approval.
To avoid these problems, the person creating the study form in iRIS should follow the steps described in pages 7 and 8 of the iRIS user manual entitled “Basics for Creating a New Study Submission- Manual 1.” The manual is available in the help section within iRIS.
FAQ about Facilitated Review – Reliance on External IRB
Q: What changes do I have to report to the UConn Health IRB when my study has been approved by an external IRB?
A: When the UConn Health IRB has elected to rely on an external IRB, the external IRB is referred to as the IRB of Record. Per the IRB Reliance Agreement in place, with one exception, only the IRB of Record for your study is responsible for all reviews of your study, inclusive of continuing reviews, requests for study modifications or amendments, and for reviews of non-compliance and unanticipated problems.
The one exception is that changes to UConn Health study personnel must still be processed through the UConn Health IRB by submitting a request for modification form through the iRIS system.
OHRP Determination of Exception to the Single IRB Review Requirements for Certain HHS-Conducted or – Supported Cooperative Research Activities Subject to the 2018 Requirements During the Coronavirus Disease 2019 (COVID-19) Public Health Emergency
To ensure that institutions conducting cooperative research are able to take advantage of the most appropriate IRB review structure, the Office for Human Research Protections (OHRP) in the Office of the Assistant Secretary for Health of the Department of Health and Human Services has determined that, for studies that are conducted or supported by HHS and subject to the 2018 Requirements, and for purposes of 45 CFR 46.114(b) (2)(ii), an exception to the requirement to use a single IRB is appropriate for the following category:
Cooperative research:
- that is ongoing or initially reviewed by the IRB during the Coronavirus Disease 2019 (COVID-19) public health emergency, as declared by the Secretary of Health and Human Services here.
- where reliance on a single IRB would not be practical; and
- for which the HHS division supporting or conducting the research approves of the use of this exception.
This exception applies for the duration of the HHS-conducted or supported research.
OHRP has made this exception determination due to concerns regarding the application of the single IRB requirement to cooperative research subject to the 2018 Requirements when this research is initially reviewed or ongoing during the COVID-19 public health emergency. The COVID-19 public health emergency has created unprecedented burdens and disruption to the research enterprise, while at the same time requiring urgent research responses that necessitate flexible approaches to oversight in order to provide vital information and to allow other research to continue where possible. This exception represents an effort to prioritize the health and safety of both research subjects and investigators, and provides flexibility to institutions in seeking IRB review due to the unique challenges created by the COVID-19 outbreak.
The exception includes some scenarios for which OHRP anticipates it may not be practical to rely on use of a single IRB for multi-site, cooperative research trials during the ongoing COVID-19 pandemic. This exception determination can be accessed here.
OHRP’s November 2019 Determination of Exception and related background information can be accessed here.
NIH Policy on Registration/Results Posting Of Basic Experimental Studies with Humans (BESH)
NIH’s clinical trial definition includes prospective basic science studies involving human participants. Basic Experimental Studies with Humans (BESH) use an intervention to understand fundamental aspects of a phenomenon without specific application towards processes or products in mind. NIH published case studies with examples of BESH (cases 9, 14, 40 & 41).
NIH funded clinical trials, including BESH, are required to register and post results in ClinicalTrials.gov.
On December 7, 2020, the Acting Director of ClinicalTrials.gov, presented the results of the National Library of Medicine analysis of challenges and considerations for registration and results information reporting of BESH in ClinicalTrials.gov. The recording of this webinar is available at https://videocast.nih.gov/watch=40141
For more information about ClinicalTrials.gov, including assistance with registration, please contact Research Compliance Monitor, Ellen Ciesielski at eciesielski@uchc.edu.
Recent Articles Published by Central IRBs
ADVARRA IRB:
Beginner’s Guide to Investigator-Initiated Trials This article describes the basic concepts an investigator must understand about “investigator initiated clinical trials” and how they fit into the clinical research landscape.
Western IRB (WCG):
Virtual Clinical Trials: Best Practices in moving Toward a Patient-Centric Research Model
This article defines virtual clinical trials, describes the potential benefits/risks of this new paradigm, and best practices for maintaining regulatory and Institutional Review Board (IRB) compliance.
Important Notice on Proposal Submission Policy
Revision Date: March 8, 2021 – revisions in italics
As an applicant organization, UConn/UConn Health has an institutional responsibility to verify the accuracy, validity, conformity, and eligibility of all applications submitted to a sponsor on behalf of the University. We have been exploring how to ensure the best delivery of services, meet sponsor and institutional policy requirements that were highlighted in the recent NSF audit, and to ensure that the University has sufficient time to review and certify proposals and increase the number of successful applications. To that end, we have conducted a survey of all faculty who submitted grant proposals within the last two years, listened to the research community’s comments at town halls, and solicited input from the President, Provost, deans, associate deans for research, the President’s Research Advisory Council, University Senate, and other faculty groups.
This listening process revealed that one of the main challenges for both investigators and staff is the bottleneck that occurs immediately prior to proposal submission. In recent years, nearly two-thirds of proposals submitted (with all components ready) are received by Sponsored Program Services (SPS) within one working day or less of the sponsor deadline.
Numerous proposals are being submitted just barely in time, meaning there is little time for a thorough review. Additionally, proposals that have been submitted to SPS far in advance also routinely lack a timely and thorough review because other proposals with an earlier deadline came in and “cut the line.”
To begin to remedy the proposal submission bottleneck, beginning May 5, 2021, the Office of the Vice President for Research (OVPR) will implement the current policy on internal deadlines for the review and submission of sponsored project proposals. The process change aims to reduce last day proposal submissions and will prioritize proposals as received. Once the policy is implemented, final administrative components of a proposal must be received by SPS Pre-Award at least five full business days in advance of the submission due date (along with a draft of the scientific components). The final submission ready proposal is due to SPS no later than noon the day before the sponsor deadline.
Exceptions include short turnaround RFPs, last minute sponsor requests, or a last minute opportunity to join a proposal under submission by another institution. Also, each UConn investigator will be given one pass to use in the event they are not able to meet the internal five-day deadline. As is the current practice, SPS Pre-Award will make every effort to submit these proposals when possible. Please visit the OVPR website for additional information and FAQs regarding the internal deadline policy.
To increase faculty support related to proposal preparation, the OVPR will be taking the following additional steps:
- The OVPR is working to address situations where investigators do not have dedicated administrative support for the preparation of a proposal; we will continue to increase staff training opportunities, extend faculty service offerings, and work to simplify the submission process.
- The OVPR will implement a dashboard to increase transparency and provide information on the status and order of review.
- The OVPR will provide additional research development services, such as grant editing and proofreading, proposal review, large and complex grant support, and research funding consultation. Further information regarding these services and how to request them is available on the OVPR Research Development section of this website.
- The OVPR will continue to work with and incorporate feedback from faculty working groups. Upon recommendation of the University Senate, the President formed a sponsored projects working group to identify impediments to the expeditious review of sponsored project proposals in advance of deadlines. The group’s report is available on the University Senate website.
Development, review, and submission timeline:
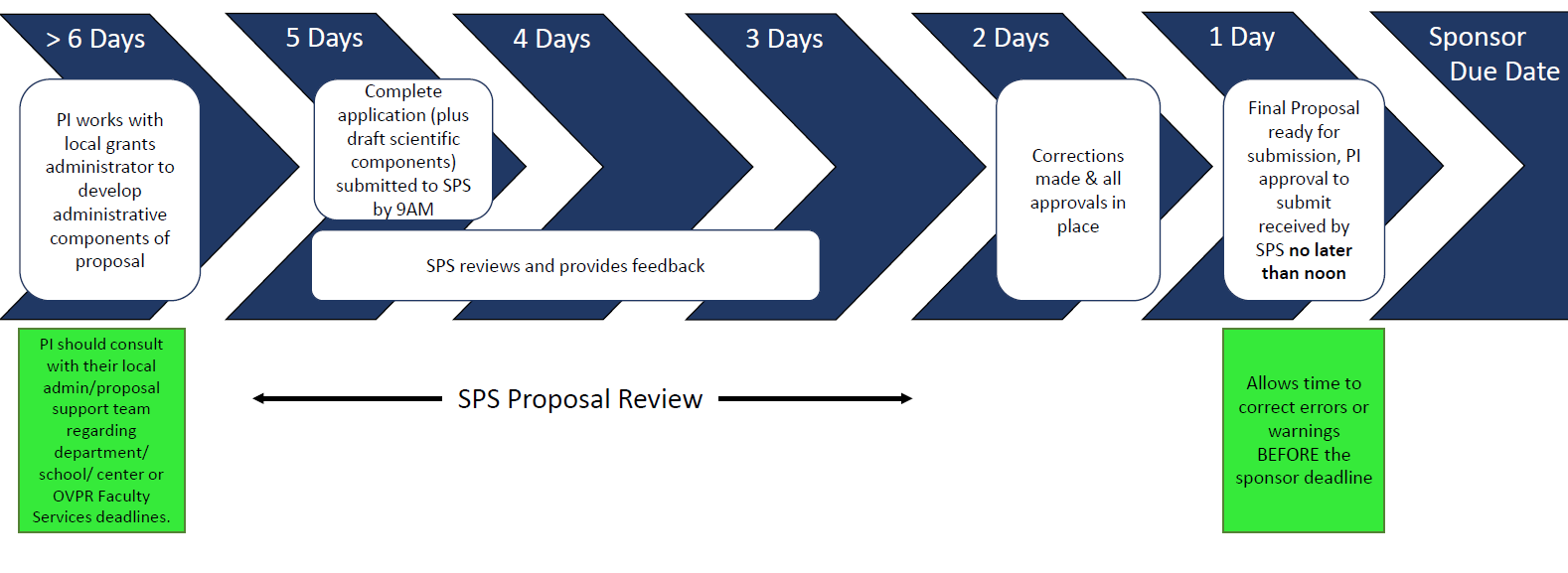
Full Business Days Before Submission Deadline
>6 days: PI provides application components to local grants administrator (or Faculty Services)
5 days: Complete application (plus draft scientific components) and IPR submitted to SPS
5-2 days: SPS reviews proposal and provides feedback
2 days: Corrections made and all approvals in place
Noon day before deadline: Final proposal and PI authorization to submit to sponsor provided to SPS
1-0 days before deadline: Proposal submitted
SPS is responsible for ensuring that applications are compliant and that institutional and sponsor guidelines are met including administrative, management, and scientific information. Please contact Paul Hudobenko (hudobenko@uchc.edu/UConn Health) or Mark Reeves (mark.reeves@uconn.edu/Storrs and Regionals) with questions as we move to a consistent and sustainable process.
Thank you for your continued cooperation in our collaborative efforts to advance UConn’s mission through innovative research, scholarship, and creative pursuits.
NIH policy on registration/results posting of Basic Experimental Studies with Humans (BESH)
NIH’s clinical trial definition includes prospective basic science studies involving human participants. Basic Experimental Studies with Humans (BESH) use an intervention to understand fundamental aspects of a phenomena without specific application towards processes or products in mind. NIH published clinical trial case studies with examples of BESH (cases 9, 14, 40 & 41).
NIH funded clinical trials, including BESH, are required to register and post results in ClinicalTrials.gov. On Monday, December 7th from 3:00-4:00 pm, Rebecca Williams, Acting Director of ClinicalTrials.gov, and Elisa Golfinopoulos will present the results of the National Library of Medicine analysis of challenges and considerations for registration and results information reporting of BESH in ClinicalTrials.gov. You may send questions before or during the event to SciencePolicy@od.nih.gov with the Subject “BESH Webinar”
Webinar: Monday, December 7, 2020 3:00-4:00 PM https://videocast.nih.gov/watch=40141
For more information about ClinicalTrials.gov, including assistance with registration, please contact Research Compliance Monitor, Ellen Ciesielski at eciesielski@uchc.edu.
HSPP- July-August-September, 2020- Newsletter
Informed Consent Process and Documentation
One of the most important aspects of conducting non-exempt human subject research is obtaining the legally effective informed consent of the subject or the subject’s legally authorized representative (LAR) before involving the subject in the research. Study personnel who will be obtaining consent should be familiar with the following IRB policies
- 2011-008.0 – Informed Consent Forms
- 2011-008.1 – Informed Consent Process
- 2011-008.5 – Informed Consent, Providing and Obtaining Informed Consent
Exceptions to the above noted policies may be granted by the IRB if certain criteria are met. Those exceptions are described in IRB policy 2011-008.2.pdf – Informed Consent, Waivers and Alterations.
The following section presents a general overview of a correct informed consent process and documentation of consent. Examples of non-compliance with the process and documentation of consent are also provided.
Informed consent process and documentation:
- The consent process occurs in a private setting.
- The consent process starts with a potential participant being given the opportunity to review the informed consent form and is followed by a discussion about the research.
- The process is free of coercion or undue influence.
- The process occurs under circumstances that provide the prospective subject, sufficient time to discuss, ask questions and consider whether or not to participate.
- Once an individual has had all his/her questions answered and has had ample time to consider the information s/he decides whether or not to participate.
- Unless documentation of consent has been waived by the IRB, the informed consent process is documented by use of an IRB approved informed consent form.
- The IRB approved consent form must be signed and dated by the subject (or legally authorized representative) and the person obtaining consent.
- All names, signatures and dates should be entered in the document on the same date and at the same time.
- After the signatures are obtained the participant must be provided with a copy of the complete signed informed consent document.
- Documentation of the initial informed consent process may be supplemented by notes in a research chart that indicate on-going discussions with the subject at subsequent study visits.
- At the conclusion of the consent process investigators should provide a Research Participant Feedback form to the subjects.
Examples of Non-Compliance with the Consent Process
- Consent for participation obtained from next of kin, spouse or other individual in a study that does not have IRB approval to obtain consent from a legally authorized representative (LAR).
- Consent obtained from individual who is not part of the approved study team.
- Research interventions occurred prior to obtaining consent.
Examples of Non-Compliance with Documentation of Consent
- Consent form is not signed by the subject
- Consent form is not signed by the person obtaining consent.
- Dates of signature are either missing, incomplete or incorrect.
- The original consent document is not retained.
- Dates contained corrections, which obscured the original entry.
- The most recent version of the approved consent form was not used when consent was obtained
Mayo Clinic Expanded Access Program (EAP) – Update
On August 23, 2020, the US Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for convalescent plasma for the treatment of hospitalized COVID-19 patients. Click here for more information regarding the Emergency Use Authorization (EUA) announcement. The Emergency Use Authorization (EUA) is currently active and represents the preferred means of administering convalescent plasma.
For additional information, please consult the US FDA fact sheet for health care providers, available at: https://www.fda.gov/media/141478/download
New patient enrollment in the Mayo Clinic EAP is not authorized after August 28, 2020.
Order of convalescent plasma under the Mayo Clinic EAP is not authorized after August 31, 2020.
Participating sites are required to complete data follow-up forms for all patients enrolled in the Mayo Clinic Expanded Access Program (EAP).
Please visit our website for additional information: Convalescent plasma therapy
Expanded Access for Treatment Use, Including Single Emergency Use – IRB Policy Update
Uconn Health‘s Human Subjects Protection Program (HSPP) policy 2011-022.2.pdf – Investigational Drug/Biologic – Expanded Access for Treatment Use, Including Single Emergency Use has been revised. This revision is to inform clinicians who intend to use the Expanded Access Program in a single emergency case that if time permits, prior to the emergency use, the prescribing clinician should complete an application for expedited review in the iRIS submission system. The application in iRIS -Section 1, should indicate the type of research as: “Expanded Access –Single Patient.”
Within the online application the clinician must also describe his/her intent to utilize an investigational drug for a therapeutic reason at least 24 hours prior to the planned date of the first administration of the drug. In addition, an email notification should also be sent to a Regulatory Specialist (RS) within the office (IRB contact information available at http://research.uchc.edu/rcs/hspp/) to alert the IRB of the situation such that the submission can be prioritized for review.
If prior review is not possible, the submission in iRIS is to be made within 5 business days of the drug administration.
Expedited review may be requested also for a single patient COVID-19 Expanded Access request for which a waiver of the requirement for full board review has been granted by the FDA in accordance with the FDA guidance that review by the IRB Chair or designee is sufficient.
The documents required for an Expanded Access Expedited submission are described in detail in the new published Application Checklist – Single Patient Expanded Access .docx
IRB Forms – Update
The Application Checklists have been updated to reference when additional approvals from I.T. may be required to ensure that data security measures are adequate.
The application checklists for Exempt status, Expedited review, Full board review and Facilitated review, now include the following requirement:
If Institutional standards for data security, inclusive of standards for use of data encryption, are not being used on all devices (e.g. desktop, laptop, thumb-drive, other mobile devices) used to store/transfer data, approval from I.T. for use of alternate data security plan. Contact Carrie Gray with questions (860) 679-2295, cagray@uchc.edu. If not provided the IRB application should indicate data encryption is being used and implies Institutional standards are being followed.
The Initial Application form in iRIS now contains this note: Study personnel must be aware of and comply with relevant IRB policies and institutional policies for data security. Links to IRB and UConn Health policies are available from the HSPP website at https://ovpr.uchc.edu/services/rics/hspp/policies/ and https://ovpr.uchc.edu/services/rics/hspp/policies/uch-policies/
Institutional data security standards, inclusive of standards for use of encryption, must be followed unless approval from I.T. to deviate from Institutional standards is obtained. Contact Carrie Gray with questions (860) 679-2295, cagray@uchc.edu
The Main Consent Form Template .doc has been revised to include text in the sections regarding confidentiality for studies that use the medical record. This was added because of the ability to share EMRs across institutions. New submissions must use the latest revised consent form template. Approved studies are not required to change their consent forms. The revision to that section includes that any clinical/provider that subjects see, whether at UConn Health or elsewhere, may potentially have access to the information in their medical record.
New FDA Guidance for Civil Money Penalties for ClinicalTrials.gov- Non-Compliance
On August 14, 2020, the Food and Drug Administration (FDA) published new guidance titled “Civil Money Penalties relating to the Clinical Trials.gov Data Bank.” The guidance clarifies how the FDA identifies whether responsible parties have failed to submit required clinical trial registrations or results to ClinicalTrials.gov, or knowingly submitted false or misleading information, and details the applicable fines, including “$10,000 for each day that the violation continues” and potential civil or criminal penalties.
Applicable clinical trials include those evaluating at least one drug, biological, or device product regulated by the FDA.
If your NIH-funded study involves human subjects, you can use the NIH decision tree to determine if it meets the NIH’s broad definition of a clinical trial and will therefore require registration and results posting.
For more information about ClinicalTrials.gov, including assistance with registration, please contact Research Compliance Monitor, Ellen Ciesielski at eciesielski@uchc.edu
New FDA Guidance for Civil Money Penalties for ClinicalTrials.gov Non-Compliance
On August 12, 2020, the Food and Drug Administration (FDA) issued a final guidance document titled “Civil Money Penalties relating to the Clinical Trials.gov Data Bank.” The guidance clarifies how the FDA identifies whether responsible parties have failed to submit required clinical trial registrations or results to ClinicalTrials.gov, or knowingly submitted false or misleading information, and details the applicable fines, including “$10,000 for each day that the violation continues” and potential civil or criminal penalties. Applicable clinical trials include interventional studies evaluating at least one drug, biological, or device product regulated by the FDA.
For more information about ClinicalTrials.gov, including assistance with registration, please contact Research Compliance Monitor, Ellen Ciesielski at eciesielski@uchc.edu.
HSPP- April- May-June, 2020- Newsletter
HSPP- April- May-June, 2020- Newsletter
The Integrated Research Information System (iRIS ) is the electronic system used by research personnel and the Institutional Review Board (IRB) for the submission and review of research projects involving human participants. On March 21, 2013, iRIS was successfully implemented. To support said implementation, one on one training of researchers as well as weekly group sessions were carried out. These training sessions are still available to all investigators as are iRIS-training manuals. To schedule a training session e-mail Mayra Cagganello (cagganello@uchc.edu). To obtain a training manual click on the Help button found in your iRIS Homepage.
This present Newsletter has been prepared to address the most common and current difficulties observed when investigators navigate the system. In the majority of the cases, these difficulties have caused delays in approval. In addition to the training options noted above, it is highly recommended that all iRIS users read this newsletter to increase knowledge of the system thus preventing delays in approvals.
The Most Common Mistakes with Revisions of Documents in iRIS
Once a submission is received by the IRB in iRIS, an IRB Regulatory Specialist (RS) conducts a pre-review of that submission. If the RS determines that corrections or additional documentation is needed before the submission can be formally reviewed by the IRB, the RS will return the submission to the study team either in a Submission Correction Form or in a Submission Response Form describing the corrections that are necessary.
The following section describes the major issues observed when investigators are submitting revised documents in the above mentioned submission forms.
Issue #1: Investigators upload revised documents to the system section for Protocol items rather than to the Submission Form .
The corrections requested must be made within the Submission form sent by the IRB (e.g., the Submission Correction Form or the Submission Response Form). The IRB does not have access to your Study’s Protocol items. The IRB will only see and review documents uploaded/attached to the Submission Forms.
Issue #2: Investigators upload edited documents to the Submission Form as brand new documents instead of creating an iRIS revision.
If a contingency requires you to revise a document that you have submitted in previous rounds, you should follow the steps found in the iRIS User Manuals to revise the documents that are in the system.
- If you have received a Submission Correction Form, please use the instructions found in the iRIS User Manual titled: Responding to a Correction Task- Manual 3.
- If you have received a Submission Response Form, please use the instructions found in the iRIS User Manual titled: Responding to a Response Task – Manual 4.
iRIS Sign –off Notifications
Once a submission form has been routed for sign off, the iRIS system generates emails to notify the research team members and principal investigator that they need to log into iRIS and apply their sign off.
Depending on whose signature is required, the e-mail sent to the study team members will have a different message.
Below are two possible messages the study team can receive when sign off are required. The subject line of the notification indicates who needs to sign off.
- A “Protocol Sign-off Notification” is sent to all members of the study team with a subject line stating: Member of Research Team – Initial Notification for Review and Signoff. In this case, all members of the study team need to log into iRIS and sign off (e.g., an initial submission application form).
The body of the email will specifically state that the study is in need of signatures from one or more team members of the team in order to continue the submission process to the IRB.
- A “Principal Investigator Signoff Notification” is sent to all members of the study team.
- However, the subject line indicates that this is a Principal Investigator Signoff Notification. In this case, the submission has been routed only to the Principal Investigator for sign off (e.g., a Response form, an initial Modification Form, Continuation Form, Problem Report Form, and Closure Form,). Even though the PI sign off is the only one required, all study team members receive the notification so that they are aware that the PI needs to do so.
The body of the email will state PI Signoff Needed.
Investigators should review the content of the notifications to determine whether to log into iRIS to sign off. Many investigators log into iRIS with the intention to sign off on a submission, however, their signatures are not required.
iRIS Frequently Asked Questions (FAQ)
Q: Who needs to request an account to access iRIS?
A: If you are affiliated to UConn Health (e.g., if you are a student, a resident, a fellow, a faculty member, or staff), by virtue of said affiliation you already have the ability to log in to iRIS. Your UConn Health network’s credentials are to be used to log into iRIS.
Individuals who are external to UConn Health (e, g., a UCONN Storrs student or faculty, a Hartford Hospital physician, etc.) who need access to iRIS should request an external account in iRIS. An online request form must be completed by clicking on the Request New Account option found in the iRIS logging page. The person requesting the account should provide an explanation as to why the account is necessary and with whom at UConn Health the researcher will be associated.
An email request to create an account in iRIS is not adequate to generate an account in iRIS. The information provided in the on-line request form is necessary to build an account for an external user. To avoid inaccurate information this online request form should be completed by the person in need of the account.
Q: I am unable to log into iRIS. What should I do?
A: Internal Users (Investigators Affiliated to UConn Health): If you are having trouble accessing iRIS with your UConn Health network credentials, please try to verify the following prior to contacting the HSPP/IRB office:
- Your network credentials are case sensitive. Check the basics such as cap lock or number lock issues.
- Ensure that your UConn Health password has not expired (you can test this by rebooting your personal computer).
- If you recently changed your password, please try rebooting your personal computer before logging into IRIS.
- Make sure you are not coping and pasting your credentials into the iRIS’s log in boxes. Your user ID and password must be typed into the iRIS log in boxes.
- If you are still experiencing problems using your UConn Health credentials, please contact the UConn Health help desk at x4400.
External Users (Investigators NOT Affiliated to UConn Health): If you are having trouble accessing iRIS with the credentials provided when your account was created, you do not need to request another account. Please, do the following:
- The iRIS accounts of external users are active for a maximum of an 18-month period. If you have not used iRIS for a long time and you think your account has expired, send an email to Mayra Cagganello ( cagganello@uchc.edu ) requesting an extension of your account.
- If your account is active ( is not expired) but you forgot your iRIS User ID, send an email to Mayra Cagganello ( cagganello@uchc.edu ) requesting your iRIS User ID.
- If you know your iRIS User ID but can’t remember your password, you will need to retrieve your password from iRIS. To do so, click on the “I forgot my Password” tab found in the iRIS logging page . Enter your iRIS User ID in the box provided, and then click on the “Send Password” tab. The IRIS system will send your password to the e-mail address found in your iRIS account.
- If you have tried to retrieve your password but have not received an email from iRIS with your password, it may be that your email address in your iRIS account is no longer valid. If you have a new email address, email your new email address to Mayra Cagganello ( cagganello@uchc.edu ) with a request to update your email address in iRIS.
Q: Who Needs to Sign off on Submissions in iRIS?
The table below explains:
| Form
|
Who is Required to Sign |
| Initial submission form for a new study | All key study personnel identified on the application form, excluding those who are listed only as a contact person.
|
| Correction form | Any member of the study team, most often the study coordinator. |
| Response form | The Principal Investigator (PI) |
| Continuation Form | The Principal Investigator (PI) |
| *Modification Form | The Principal Investigator (PI) |
| Problem Report Form | The Principal Investigator (PI) |
| Closure Form | The Principal Investigator (PI) |
| When only the PI is required to sign the form on the routing sign-off sheet, the boxes next to the names of the other key study personnel should be unchecked.
*When new personnel are being added to the study through a request for modification, they will be asked by the IRB to sign off as a contingency for approval.
|
|
When a Submission form is routed for sign off and other members of the study team are checked for sign-off, you should uncheck the boxes next to their names to deselect them as shown in the screen shot below. Likewise, initial continuations, modifications, problem reports and closure forms only require the Principal Investigator (PI) sign off. If other members of the study team are listed in the routing sign off sheet, you can uncheck the boxes to deselect their names .
Q: I am submitting a modification form to add new personnel to an approved study. However, when routing the modification form for sign off I am unable to find the name of the new investigators in the Sign off Submission Routing list.
A: When a Modification Form is created in iRIS, such form works as a “request” made to the IRB. Only principal investigators are required to sign off on an initial Modification Form.
When routing this form for sign off, the investigator working on the form will not find the names of the new personnel in the Sign off Submission Routing list. This is because this request will be granted after the IRB has verified that the new personnel has complied with the human subjects protection training (e.g., CITI Training) requirement. Moreover, the iRIS the system verifies whether the new added personnel has a valid iRIS account.
After the IRB staff and IRIS system have confirmed that the new personnel has met these requirements, an IRB Regulatory Specialist will add the names of the new personnel to the Key Personnel section of the study allowing the new investigator access to the study.
The IRB Regulatory Specialist then returns the Modification Form to the study team in a Correction Form with a contingency for approval. The contingency will require that the new personnel sign off to accept his/her role in the study. At this point, the study team working in the Correction Form will find the names of the new personnel in the Sign off Submission Routing list.
Q: I routed a submission form to the IRB a while ago. I have not hear from the IRB. I see that the track location of the form states that is “Waiting for Finalization of Routing List.” What should I do?
A: In order for a form to arrive to the IRB queue in IRIS, the person submitting the form must complete several steps to route the form for sign off. When all sign offs on the form have been completed, the system moves the submission form to the Submission box of the IRB in IRIS.
Whenever an investigator sees a yellow square under the “Track Location” that means that the form built in iRIS was never routed for sign off .
In the example below, the submission Correction Form is waiting for someone from the study team to route the form for signatures.
To route the form to the person who has responded to the contingencies, the following steps must be completed. Begin by clicking click on the magnifier glass located on the yellow box under the Track Location. Second, click on the “Routing Assignment List” (icon with the two heads). Manually uncheck the boxes next to the names of the other members of the study team to deselect them. Then, click on Save and continue twice. If you are not the person who needs to sign off, log out. The submission will be in the iRIS homepage of the person whose signoff is required.
If you are the person who needs to sign off you will see the “approve” radio button. Click on the approve radio button and enter your credentials to sign off. Finally, click on Save to save your sign off.
Q: How do I know if the IRB received my submission.
A: Your submissions forms are in the IRB inbox in iRIS when you see a green box under the Track Loction stating “Routing in Process.”
New iRIS users should use the iRIS User Manuals to ensure all the steps for routing submissions to the IRB have been completed.
Informational Session/Q&A on Research at UConn During & After the Pandemic
SAVE THE DATE: The Office of the Vice President for Research will join President Thomas Katsouleas in hosting a virtual informational session for UConn & UConn Health researchers on Monday, April 20 from 11:00am to 12:30pm. The purpose of the session is to update the UConn research community on critical information related to research on campus during and after the COVID-19 pandemic, as well as answer questions from UConn faculty and staff. A number of questions have already been submitted via the University Senate. If you would like to pose a question regarding our research activities or share a comment, please send it to ovpr@uconn.edu before Monday, April 20.
While the world is still in the midst of the ongoing crisis, there are a great many unknowns when it comes to research and our other operations, but participants will endeavor to answer every question they are able to and discuss what is known with respect to research as of April 20.
A communication with a web address on how to watch and participate in the town hall will be sent later this week.
OVPR Internal Funding Announcement
Dear Colleagues,
I hope this message finds you well, as we have all been facing many challenges related to the COVID-19 epidemic over the last several weeks. While our focus has been on rapidly shifting to new methods for teaching and conducting research, the Office of the Vice President for Research (OVPR) is pleased to announce that decisions for several of our internal funding programs have been finalized. These programs support a variety of high impact research, scholarship, and artistic pursuits across UConn and UConn Health’s departments. The OVPR is thrilled to support these diverse projects, which will lead to additional extramural funding and increase the reputation of UConn amongst peers. Funding for the following recipients will be made available now for projects that can be conducted remotely, and will be on hold for other recipients until the University resumes normal operations after the COVID-19 pandemic. Decisions regarding other internal funding programs including the Research Excellence Program (REP) and Scholarship and Collaboration in Humanities and Arts Research (SCHARP) are expected to be announced in May.
Please join me in congratulating winners for the following funding programs and visit the OVPR’s Internal Funding website to learn more about these programs:
Convergence Awards for Research in Interdisciplinary Centers (CARIC)
CARIC is an initiative of the Office of the Vice President for Research (OVPR) that provides support of up to $150,000 for the development of collaborative interdisciplinary teams to bid for major (>$5M) federally funded initiatives, such as research centers. CARIC provides funding for planning, outreach to strategic partners, and proof-of-concept research activities that will prepare the team to bid competitively for these prestigious federal awards.
Puxian Gao, Material Science and Engineering
Mapping Catalytic Energy Transformations: Convergence of Nanoarray Catalysis, In Situ Microscopy, and Data Science
Jeffrey Hoch, Molecular Biology and Biophysics
Biomolecular Digital Commons
Cato Laurencin, Connecticut Convergence Institute
Convergence Center for Regenerative Engineering- A Science and Technology Center
Mark Urban, Ecology and Evolutionary Biology
241: Reintegrating Biology & Harnessing the Data Revolution to Predict and Prevent Global Ecosystem Change
Microbiome Seed Fund Recipients
Through this program, the OVPR is able to provide up to $50,000 to UConn faculty to support innovative and collaborative research projects that will lead to new proposals for extramural funding in microbiome research.
Jonathan Klassen, Molecular and Cell Biology
Metal-Binding Antimicrobial Peptide Mediation of a Fungus-Growing Ant Symbiosis
Co-PIs: Alfredo Angeles-Boza
Mark Peczuh, Chemistry
Characterizing the Role of Siderophores in the Euprymna Scolopes – Vibrio Fischeri Symbiosis
Co-PIs: Spencer Nyholm
J Evan Ward, Marine Sciences
The Effect of a Common Anthropogenic Pollutant on the Microbiome of an Ecologically and Commercially Important Bivalve
Co-PIs: Penny Vlahos, Lisa Nigro
Wing Ki Mok, Molecular Biology and Biophysics
Friend or Foe? Impact of Chronic Infection Microbiome Constituents on Persistence of Staphylococcus Aureus toward Antifolate Antibiotics
Co-PIs: Dennis Wright, Maria Rocha Granados, Debjani Si
Spring 2020 Scholarship Facilitation Fund Program
Through this program, the OVPR is able to provide up to $2,000 to UConn faculty across all disciplines, on a competitive basis, to foster, support, and enhance research, scholarship, and creative endeavors. (Please visit the site for the full list of recipients.)
START Preliminary Proof-of-Concept Q1-3
Through this program, the OVPR is able to provide up to $10,000 to Central Connecticut State University, Southern Connecticut State University, University of Bridgeport, and UConn faculty to foster and bolster the initial validation of innovative early stage technologies that have possible commercial potential. The program is designed to bring these promising technologies to a stage that may be more attractive for additional later stage translational funding support. (Please visit the site for the full list of recipients.)
Cheers,
Radenka
COVID-19: NSF RAPID Program Opportunities
Dear Colleagues,
While we all face turmoil caused by the global coronavirus pandemic, I wanted to make sure that all faculty are aware of unique funding opportunities through the National Science Foundation with the specific aim of helping address COVID-19. Specifically NSF’s RAPID funding mechanism allows for a drastically reduced submission/award timeline to address this urgent need. Please see the Dear Colleague letter below from NSF Director, Dr. France A. Córdova for more information and consider applying through this mechanism if you are conducting applicable research.
Thank you, as always, for your continued support of UConn and our research community.
Sincerely,
Radenka
NSF 20-052
Dear Colleague Letter on the Coronavirus Disease 2019 (COVID-19)
March 4, 2020
Dear Colleague,
In light of the emergence and spread of the coronavirus disease 2019 (COVID-19) in the United States and abroad, the National Science Foundation (NSF) is accepting proposals to conduct non-medical, non-clinical-care research that can be used immediately to explore how to model and understand the spread of COVID-19, to inform and educate about the science of virus transmission and prevention, and to encourage the development of processes and actions to address this global challenge.
NSF encourages the research community to respond to this challenge through existing funding opportunities. In addition, we invite researchers to use the Rapid Response Research (RAPID) funding mechanism, which allows NSF to receive and review proposals having a severe urgency with regard to availability of or access to data, facilities or specialized equipment as well as quick-response research on natural or anthropogenic disasters and similar unanticipated events. Requests for RAPID proposals may be for up to $200K and up to one year in duration. Well-justified proposals that exceed these limits may be entertained. All questions should be directed either to a program officer managing an NSF program with which the research would be aligned or to rapid-covid19@nsf.gov.
Complete guidance on submitting a RAPID proposal may be found in Chapter II.E.1 of the NSF Proposal and Award Policies and Procedures Guide.
We ask that all investigators and organizations maintain awareness of the dynamic nature of this event through regular monitoring of official communications from the Centers for Disease Control and World Health Organization.
NSF has also provided Frequently Asked Questions that address questions associated with NSF proposal submission and award management relevant to research proposals relating to COVID-19 as well as possible impacts of COVID-19 on activities under existing awards and on participation in NSF’s merit review panels; that website will be updated as appropriate.
Sincerely,
Dr. France A. Córdova
Director
Research Shut Down Notice March 23, 2020
With Governor Lamont’s order for all non-essential businesses to suspend operations, the president, provost and vice president for research have determined that all on-campus research activities on ALL CAMPUSES – UConn, regional and UConn Health – must stop and labs must
close by 8 p.m. on Monday March 23.
In addition to faculty, this includes research being conducted by undergraduates, graduate students, and postdoctoral scholars. The only exceptions to this are human subjects clinical trials, research where continued in-person interaction or intervention is needed for the safety and welfare of enrolled subjects, research that is directly connected to addressing the COVID-19 crisis, and research that can be conducted remotely by faculty, staff, and/or students without in-person intervention or interaction with research subjects.
We understand the enormous impact this decision will have on faculty and students. But as we deal with the challenges of a global pandemic as well as the uncertainty of its impact on all aspects of the University and surrounding communities, we must make difficult decisions guided
by the principles of health and safety.
- Faculty and research staff should follow the Laboratory Ramp-Down Checklist: Procedures for Safely Vacating a Laboratory (updated March 22, 2020) to close down their research and labs.
- Research related to COVID-19 can continue, but faculty must submit a Critical Research Infrastructure Inventory form indicating they need to begin or continue this work and describe the work (see last question on the form).
- Faculty with animals must contact the attending veterinarian for their campus regarding steps to immediately reduce animal numbers and number of cages. Breeding must be reduced to the minimum possible; no increases in cage counts will be permitted and plans should be in place for reductions of cage counts in the future. Labs using aquatic, avian, or other species that are housed outside the vivarium must contact the attending veterinarian regarding how animal care and husbandry operations will be maintained.
- Any faculty with critical research infrastructure, such as unique reagents, unique cell lines, equipment, liquid nitrogen stocks, and certain long-term experiments should complete the Critical Research Infrastructure Inventory form (updated March 22, 2020). These will be reviewed and the faculty
member will then be advised on how to proceed based on their individual situation. - Any researcher or faculty member who is unable to halt their research by Monday’s deadline or who has a unique situation that needs to be considered should email ovpr@uconn.edu with a description of the situation or need and their recommendation for how it can best be met or addressed. The email should include a phone number(s) where the faculty member can be reached.
- Any student or employee who feels they have been asked unreasonably to continue on campus research beyond Monday’s deadline should contact the dean of their school or college and the OVPR without fear of retaliation.
For now, the shut-down of labs will be in effect until April 22, 2020. We will assess and monitor the status as events change daily. However, you should plan for a remote-work research operation and lab closure that could last for several weeks or months.
HSPP-January-February-March, 2020 – Newsletter
Office of the Vice President for Research (OVPR)
COVID-19 Guidance for the UConn Health Research Community
The Office for the Vice President for Research (OVPR) website has posted a COVID-19 Guidance for the research community at UConn Health. Information about the impact and changes caused by the COVID-19 outbreak on research activities are described on this guidance. Information on this web site is updated frequently.
IRB Policies – Revisions
IRB Policy 2011-015.0. -Recruitment and Payment and policy 2011-011.0- Research Personnel have been revised to better outline the requirements and expectations for recruitment of UConn Health patients. The policies denote, among other items, that the person who first approaches a patient about research participation must be someone with an existing treatment relationship with the patient and that members of the study team (e.g., principal investigators, co-investigators, study coordinators, consenters, etc.) interacting with the patient-participant must be affiliated with UConn Health (e.g. faculty appointment, employee, student, intern, volunteer).
If the study submitted for review has a Principal Investigator who is not a paid UConn Health faculty member, there must be a paid faculty member from UConn Health as a co-investigator on that study who is responsible for patient involvement.
IRB Forms – Update
The following forms have been revised:
- Consent checklist – Addendum for Genetic Research – This form was revised to clarify wording and to re-order the elements of consent.
- Main Consent Checklist – This form was revised to add elements for inclusion of any requirements imposed by a specific funding Institute, Office or Center within NIH related to data sharing (added in the NIH section of the checklist)
- Main Consent template – This template was revised to add instruction for investigators to check whether the funding entity has any specific requirements regarding data sharing language and if so to include it. The NIAAA suggested language was provided as an example.
Connecticut Law Raises Legal Age to Buy Smoking Products to 21
As of October 1, 2019, the State of Connecticut change the legal age for smoking from 18 to 21. UConn Health investigators who are conducting studies with tobacco products should review their studies and as needed revise them to comply with this new law in Connecticut.
NIH Update: Guidance for NIH-Funded Clinical Trials and Human Subjects Studies Affected By Covid-19
The National Institute of Helath ( NIH) has published the following guidance NOT-OD-20-087 outlining the flexibilities available to recipients impacted by COVID-19 for delays to ongoing research, delays to research progress for NIH-funded clinical trials and human subject studies, and unanticipated costs.
Disclosure Form for Work Submitted to Medical Journals
As stated by Darren B. Taichman, MD, PhD; Joyce Backus, MSLS; and Christopher Baethge, MD; et al, in their published article titled “A Disclosure Form for Work Submitted to Medical Journals. : A Proposal from the International Committee of Medical Journal Editors” the International Committee of Medical Journal Editors (ICMJE) adopted the “ICMJE Form for the Disclosure of Potential Conflicts of Interest” as a mechanism for collecting and reporting authors’ relationships and activities that readers might consider relevant to a published work.
The ICMJE has proposed changes to this disclosure form to enhance transparency and accuracy in the information captured by this form. The ICMJE is requesting feedback about the proposed new form. Comments received by April 30, 2020 will be consider for the finalization of the revised version. The current ICMJE Form for the Disclosure of Potential Conflicts of Interest is available and downloadable in PDF at their website. To enter your comments on the proposed form, please click here.
Recent Articles Published by Central IRBs
ADVARRA IRB:
Key Biosafety Considerations for Coronavirus Research: This article provides an overview of the coronavirus and describe strategies for developing medical countermeasures to combat the recent outbreak. A description of the opportunities, risks, and risk mitigation strategies for coronavirus are also discussed in this article.
Beyond the Regulations: More Considerations for Emergency Research: this article describes what the researchers and research organization must know about “Emergency Research.” The authors explain emergency research is only feasible if a plan is in place. These plans include but are not limited to the establishment of a front-line staff communication plan, an evaluation of clinical operations, and a plan to respond to media inquiries.
Western IRB (WCG):
“Your 5 Questions About Enrollment Assistants Answered”: In this article WCG describes the services they provide through “Enrollment Assistants” (EAs) for recruitment, and enrollment in clinical studies. Mark Summers, president of patient engagement from WCG addresses the following questions: (1) how can a person from outside the study team legally work at a site? (2) How accepting are sites of EAs–especially sites that have never worked with one? (3) Are EAs trained onsite or by WCG Three Wire? (4) Would an Enrollment Assistant be more beneficial to, say, a large academic center than to a small standalone research site? (5) How do you keep track of your enrollment performance metrics?
“COVID-19 Preparedness for Health Care Institutions: Insights” Paul Biddinger, MD and Scott Gottlieb, MD: This article is a summary of takeaways and key points from the March 13, 2020 webinar sponsored by WCG.
Important NIH teleconference on Covid-19 Monday, March 16, 2020
Dear UConn Community,
Research!America is hosting a conference call on Monday, March 16th from 1:30 to 2:30 PM with NIH Deputy Director Lawrence Tabak. Dr. Tabak will discuss NIH’s efforts to ensure research institutions and scientists are accorded the flexibility needed as they confront COVID-19-related research disruptions. No need to RSVP for the call (call number below). To dial in:
What: Teleconference with Dr. Larry Tabak
When: 1:30-2:30 p.m. ET, Monday, March 16, 2020
Call-In: 866-876-6756 (toll-free) or 704-288-1165 (U.S.)
Passcode: 737857
The following are additional updates and guidance from the NIH and NSF
o Frequently Asked Questions (FAQs) about COVID-19 for the National Science Foundation
o NSF website for the research community with detailed guidance on the Coronavirus (COVID-19)
o Frequently Asked Questions (FAQs) about COVID-19 for the National Institutes of Health
Cheers,
Radenka
Attention- UConn Health Human Subjects Research Community:
The UConn Health Institutional Review Board (IRB) would like to remind Principal Investigators (PI) and study personnel of existing IRB policies and procedures that are in place and that may be relevant given the potential impact of COVID-19 on research. Because every research protocol is different, the IRB is not issuing a single standard. Principal Investigators are responsible for the oversight of their research, for knowing the nature of their research, and for determining what action, if any, is needed for ensuring appropriate policies and procedures are followed. The following policies may be of particular relevance during this time. Principal Investigators and study personnel should review these policies and determine which actions, if any, are appropriate.
Policy 2011-009.1 – Institutional Review Board – Submission of Materials: In accordance with this policy, if a Principal Investigator determines that a change to the implementation of the protocol is necessary, a request for modification is to be submitted to the IRB. For example, if the PI determines that all subject interviews will be conducted by phone vs. in person, a request for modification should be submitted to the IRB. As with any modification, the change should be clearly described to the IRB. For example, changes that will only occur for a limited timeframe should be described accordingly (e.g. “while the COVID-19 pandemic is ongoing, subject interviews will be conducted by phone whenever possible”). When possible, approval for such changes is to be received prior to the change being implemented. However, if a change in protocol is required to eliminate apparent immediate hazards to subjects, the PI may implement that change and report it to the IRB within five business days. In this type of situation, the change to protocol would be anticipated to be a lasting change and not particular to one subject ,which would be reported per one of the following policies.
Policy 2009-002.0 – Reporting Non-Compliance to the Institutional Review Board: In accordance with this policy, protocol deviations within the control of the research team are to be reported to the IRB within five business days. Non-compliance that is not within the control of the research team and that does not pose risks to subjects is to be reported to the IRB at the time of continuation or study closure, whichever comes first. For example, if a subject declines to come to a study visit due to general concerns about COVID-19, and missing that visit will not place the subject at risk, this would be tracked by the study team and reported to the IRB at study continuation or closure. Likewise, if the institution makes a policy decision that prevents the study team from fully implementing the approved protocol, the deviations would be tracked and reported at study continuation or closure, provided the subjects were not put at risk. For example, if the institution limited access to only those providing or needing clinical care, subjects would not be able to come on site for interview/survey procedures. It is anticipated that the tracking of protocol deviations will be the most prevalent course of action during the COVID-19 pandemic.
Policy 2009-001.0 – Reporting Unanticipated Problems to the Institutional Review Board: An unanticipated problem is any unforeseen occurrence that involves risk to the subject or others, and that is related to or is possibly related to either a research intervention or interaction, or the conduct of the study in general. If a protocol is not able to be implemented and that inability places the subject at risk (e.g. subjects prevented from coming to institution to receive clinical research intervention and the lack of intervention puts the subject at risk), the PI should report this to the IRB. This may be a single missed visit; or it may become a concern after a certain number of visits are missed.
In summary, it is the responsibility of the Principal Investigator to oversee the implementation of the research protocol within the framework of existing IRB policies and procedures. If you have any questions, you may contact one of the IRB Regulatory Specialists.
- Steven MacKinnon for IRB numbers ending in -1 or .1 (mackinnon@uchc.edu, 860-679-8729)
- Patricia Gneiting for IRB numbers ending in -2 or .2 (gneiting@uchc.edu, 860-679-4849)
NSF 2026 Idea Machine
Dear Colleagues,
In the summer of 2018, the National Science Foundation (NSF) launched an innovative competition, the NSF 2026 Idea Machine, to crowdsource big challenges and big ideas that could help tackle them. The Idea Machine aimed to set the stage for breakthrough research in science, technology, engineering, and mathematics (STEM) and STEM education through the nation’s 250th anniversary in 2026 and beyond. NSF received around 800 entries from established researchers, students, teachers, and even high school and middle school students from all across the country. Those 800 big ideas have now been narrowed down to seven finalists, which were announced last week.
As we continue to work towards fulfilling President Katsouleas’ bold vision to boost research, scholarship, and creative works at UConn, I encourage you to visit the NSF 2026 Idea Machine site and learn about the program’s goals and the recently selected finalists. This provides UConn’s research community with an opportunity to see what is next for the NSF’s long-term agenda and align our activities based on our existing and emerging strengths.
Thank you for your continued commitment to grow UConn’s profile in research, scholarship, and the arts.
Cheers,
Radenka
Dr. Radenka Maric
Vice President for Research, Innovation and Entrepreneurship
UConn/UConn Health
Professor in Sustainable Energy
438 Whitney Road Ext., Unit 1006
Storrs, CT 06269
Storrs: 860.486.3621
UCH: 860.679.2230
research.uconn.edu
HSPP- October – November – December, 2019- Newsletter
Regulatory Framework for Research with Mobile Applications
The following information was drawn in large part from the CITI Program’s module titled “Mobile Apps and Human Subject Research.” The content of this module is copyright. Uconn Health obtained permission to use this module from the CITI Program.
A mobile application (mobile app or app) is a type of application software designed to run on a mobile device, such as a smartphone or tablet computer. Medical mobile apps (MMAs) are medical devices that are mobile apps, meet the definition of a medical device and are an accessory to a regulated medical device or transform a mobile platform into a regulated medical device.
Research with apps may be subject to multiple federal regulations such as 45 CRF 46 (The Common Rule), the U.S. Food and Drug Administration (FDA) regulations (including 21 CFR 11), and the Health Insurance Portability and Accountability Act (HIPAA) rule. Specifically, the FDA regulates mobile health technologies that meet the definition of a medical device. When a covered entities or business associates use software and mobile applications store or transmit protected Health information (PHI) this falls within the jurisdiction of the Office of Civil Rights (OCR) under the Department of Health and Human Services (HHS). Researchers may use the information provided on the FDA website to determine if an app meets the definition of a medical device regulated by the FDA. Researchers may use the interactive tool developed by the Federal Trade Commission (FTC), in conjunction with HHS, the Office of the National Coordinator for Health Information Technology, the OCR, and the FDA to determine which laws apply to mobile health applications
When using apps in research investigators should consider the following points:
- If Consent occurs via an app the investigator should be aware that the consent document must contains all the required elements required by the Common Rule. The risk of hacking posed by the electronic consent is to be described in the consent document.
- The requirements of the IRB for an electronic informed consent process are described in the IRB Policy # 2011-008.1.pdf – Informed Consent – Process –page 4.
- Ample time to contemplate participation and ask questions will also be applicable to electronic consent, therefore app-based consent should contain a functionality to satisfy this requirement described in the IRB Policy # 2011-008.5.pdf – Informed Consent – Providing and Obtaining Informed Consent
- Because mobile apps may use, collect, store, and share data, researchers should communicate the risks of the mobile device security to the subjects and the measures in place to minimize the chance of a breach of confidentiality. If a mobile app is being used to collect protected health information the researcher must obtain an assessment from UConn Health’s I.T. department that the app is HIPAA compliant.
- The “Terms of Services” (TOS) and/or “End-User License Agreements” (EULAs) associated with the mobile apps, and devices are between the user and the service/provider, not the user and the researchers. Agreeing to TOS/EULA is different from consenting to participation in research. These agreements may require review by the IRB because they are materials for the subjects, and may include information that would affect a subjects’ decision to enroll in a study. Differences between these documents and the consent form should be communicated to the subject.
- When the research may result in collection of incidental data (e.g. use of a mobile fitness app), the researchers must indicate to the IRB what incidental data they may collect, and if this data will be disclosed to subjects. In addition, investigator should clarify whether they will keep that data and if so provide the plans to protect that data.
UConn Health Institutional Policy for Mobile Devices & Consequences of Non-Compliance with HIPAA Rules
According to UConn Health Institutional Policy # 2008-03 – Mobile Computing Devices (MCD) Security, confidential or restricted data is not authorized to be stored on either a UConn Health or non-UConn Health Mobile Computing Devices ( MCDs) unless all the criteria below are met:
- The device stores only the minimum data necessary to perform the function necessitating storage on the device.
- Information is stored only for the time needed to perform the function.
- The device requires a password for access and is encrypted using methods authorized by the UConn Health IT Department.
In addition, users may not bypass or disable UConn Health required security mechanisms, and unauthorized physical access, tampering, loss or theft of an MCD must be reported to UConn Health Public Safety.
Failure to adhere to this institutional policy and associated procedures may result in sanctions as per applicable UConn Health policy. Failure to adhere to this policy could also lead to monetary fines imposed by the Office of Civil Rights should a breach occur. For example, the University of Rochester Medical Center ( URMC) filed a breach reports with the Office for Civil Rights (OCR) of the U.S. Department of Health and Human Services (HHS) in 2013 and 2017 following its discovery that protected health information (PHI) was impermissibly disclosed through the loss of an unencrypted flash drive and theft of an unencrypted laptop, respectively. To settle the violations of the Health Insurance Portability and Accountability Act (HIPAA) privacy and security rules, the URMC agreed to pay $3 million to the Office for Civil Rights and follow a corrective action plan. A description of their corrective action plan and the two years of compliance monitoring have been posted in the HHS website.
To learn the provisions/controls defined by UConn Health IT Security when using institutionally owned devices or personally owned devices and the MCD’ user responsibilities, please review the Mobile Computing Devices (MCD) Security Institutional Policy # 2008-03.
Clarifying the CDA Process: A Researcher’s Guide to Handling Confidentiality Agreements
By Dr. Cherron Payne, Esq.
Introduction
The administration of a research study may be an arduous process for researchers and staff. Moreover, the legal aspect concerning research agreements may also be equally perplexing. Thus, this article is intended to clarify the proper procedure for handling confidentiality agreements.
Confidentiality Agreements
The nomenclature of confidentiality agreements is varied; some agreements are called confidential disclosure agreements, non-disclosure agreements or NDAs, and mutual disclosure agreements. Although the title of the agreement may vary, the agreement serves the general purpose of protecting the confidential information that is disclosed by research sponsors. Confidentiality agreements will hereafter be referred to as a “CDA”.
Before a study commences, the sponsor needs to disclose information for the researcher to evaluate his or her interest in the study. The disclosed information is often confidential because it contains proprietary information or trade secrets often in the form of models, prototypes, notes, diagrams, documents, reports, memoranda, and other forms of intellectual property. Therefore, it is imperative that researchers manage confidential information in accordance with the terms and expectations of the CDA. A researcher’s failure to properly safeguard confidential information may impose serious legal ramifications upon UConn Health. Moreover, breaching the terms of a CDA, or improperly disclosing confidential information, may also cause study sponsors to cease sponsoring UConn Health’s research.
Procedural Steps for Researchers
In order to avoid legal pitfalls, there are specific steps that a researcher or principal investigator “PI” must follow when a confidentiality agreement is received.
- The PI should first e-mail the CDA to the proper contract specialist. The PI should also e-mail the research sponsor’s contact information to the contract specialist. If the researcher is uncertain as to the appropriate contract specialist, then the researcher may contact Sponsored Program Services at 860-679-4040, by e-mail at sps@uchc.edu, or by reviewing the website of the Office of the Vice President for Research at https://ovpr.uchc.edu. The PI should never sign a CDA or agree to its terms without a contract specialist negotiating the agreement.
- If a PI receives a research study agreement without receiving a CDA, the researcher should (a) ask the study sponsor to send a CDA or (b) ask the contract specialist to request the CDA. The study agreement should not be negotiated before the CDA has been negotiated and signed.
- While negotiating the CDA, the contract specialist may have questions for the researcher or may require additional information. Researchers must furnish said information in a timely manner to avoid a delay in the negotiation.
- After the CDA has been negotiated, it is sent to the principal investigator for signature. The PI should read the agreement before signing, in order to be cognizant of the CDA terms and to properly safeguard confidential information. If there are any questions regarding the terms of the agreement, a PI may ask the following contacts for clarification: (a) the contract specialist, (b) the Director of Sponsored Program Services at hudobenko@uchc.edu, or (c) the Executive Director, Sponsored Program Services and Faculty Services at laura.kozma@uconn.edu.
- After the CDA has been reviewed, the researcher signs the agreement and promptly returns it to the contract specialist.
When the contract specialist receives the fully executed CDA, a copy will be returned to the researcher or the research staff. A fully executed copy of the CDA should be retained by the researcher to ensure compliance with the agreement.
Recent Articles Published by Central IRBs
ADVARRA IRB:
Reporting to the IRB: What NOT to Report: This article provides an overview of what the regulations do and do not say about IRB reporting requirements.
Should Social Media Be Part of Your Research Toolbox? This article discuss the benefits, the risk and the applicable regulatory requirement when using social media for recruitment and retention:
Western IRB (WCG):
An Overview of the Recent SACHRP Recommendations Around Payments in Clinical Research The U.S Department of Health and Human Services Secretary’s Advisory Committee on Human Research Protections (SACHRP) has approved two sets of recommendations regarding payments in research. The first set of recommendations identified a number of considerations for IRBs when evaluating the acceptability of incentives payments. The second set of recommendations addresses those studies that ask potential research participants to bear some or all of the cost of the research. SACHRP’s issued several questions prospective subjects and IRBs should ask when participants are required to pay for access to the experimental intervention.
IRB Forms – Update
The Pharmacy section of Appendix A.to the application and the application checklists have been revised to reflect the change in pharmacy contact to Jennifer Czerwinski, 860-679-2085, jczerwinski@uchc.edu
The HIPAA Request for Alteration or Waiver of Authorization.doc was modified to allow a brief description of the PHI to be used/accessed with reference made to documents within the submission that describe the information in more detail.
The HIPAA authorization form was revised to delete reference to the Office of Research Compliance as it is no longer a stand-alone office and to change reference to John Dempsey Hospital to UConn Health and to change HSPO to HSPP.
The Human Subject Research Determination form was revised to provide more instruction regarding the attachment of documents related to the funding source of a project.
The instructions for reliance on ADVARRA IRB were revised to reflect changes to the consent language template and the instructions for reliance upon WIRB were revised to add reference to the site number assigned to UConn Health.
Why should I register my study on ClinicalTrials.gov?
- If you wish to comply with the ICMJE policy (followed by the BMJ, JAMA and many others journals) requiring registration as a condition of consideration for publication, you may voluntarily register your study with ClinicalTrials.gov. You must register prior to subject enrollment.
- If your clinical trial is NIH funded, in whole or in part, you are required to register the study and report results on ClinicalTrials.gov.
- If your clinical trial is funded by a Federal department or agency, the Revised Common Rule requires that your consent form be posted on a public platform, like ClinicalTrials.gov, after the trial is closed to recruitment, and no later than 60 days after the last subject visit.
- If your clinical trial evaluates at least one drug, biological, or device product regulated by the FDA (See this decision checklist for more details), regardless of funder, you are required to register and post results on ClinicalTrials.gov.
For assistance with ClinicalTrials.gov, see our webpages and contact UConn Health’s ClinicalTrials.gov Administrator, Ellen Ciesielski (860.679.6004) in Research Integrity and Compliance Services.
Research Advertisement Reminder
All methods and materials to recruit participants for research require IRB review prior to implementation. Please be sure all recruitment materials (e.g., text of announcement) are IRB-approved before submitting an announcement for publication. Announcements must include IRB# and name of approving IRB (if not the UConn Health IRB). For guidance, visit: UConn Health IRB and Guidelines for submitting recruitment announcements
Export of Research Materials Abroad
To the UConn/UConn Health research community:
The Council on Government Relations (COGR) has issued an alert regarding recent situations where researchers have attempted to export research materials abroad. The FBI and other federal law enforcement agencies have increased their surveillance efforts to identify transport of research materials and verify that those exports comply with federal laws. These efforts are believed to be part of a nation-wide enforcement action to control the transport of biological materials that may present a threat to our national security and/or reduce the theft of intellectual property developed in the US, much of it with federal funds.
Transporting certain materials may require import/export permits or other documentation from federal agencies, including US Customs and Border Protection (CBP), the FDA, USDA, Fish and Wildlife, and the CDC.
Anyone with questions should contact the applicable federal agency or the UConn Export Control Office (exportcontrol@uconn.edu) for assistance.
Related news:
– https://www.universalhub.com/2019/chinese-cancer-researcher-not-allowed-leave
– https://www.universalhub.com/2019/chinese-researcher-nabbed-liquid-filled-vials
Wesley G. Byerly, Pharm.D.
Associate Vice President
NIH Asks For Your Feedback
The Office of the Vice President for Research would like to share some information regarding data sharing with researchers who may be affected.
The National Institutes of Health (NIH) is requesting comments on the draft NIH Policy for Data Management and Sharing and Supplemental Draft Guidance.
NIH will be hosting an informational webinar on the draft NIH policy and guidance on Monday, December 16th from 12:30-2:00 PM ET. The purpose of the webinar is to provide information on the draft policy and answer questions about the public comment process.
Submit your comments to NIH by January 10, 2020. Additional information can be found in this NIH blog post. Questions about the draft may be sent to the NIH Office of Science Policy at SciencePolicy@od.nih.gov.
For questions, please contact Research Compliance Monitor, Ellen Ciesielski at 860.679.6004.
HSPP-July-August-September, 2019 Newsletter
Managing Research Studies
Managing research studies efficiently and effectively requires leadership, planning, collaboration, and communication.
The Principal Investigator (PI) is responsible for the overall management of an approved study. Management of a study encompasses the ethical, technical, administrative and fiscal elements of the research study.
The PI is responsible for ensuring that the research team is oriented to the protocol and aware of their responsibilities. The study team should have specific details about the plans to accomplish the goals and procedures of the study, inclusive of plans for recruitment, consenting of subjects, data and safety monitoring, and protections for privacy and confidentiality.
The PI is also responsible for ensuring that adequate resources are available to conduct the study, including equipment, supplies, and storage space at UConn Health and in any outpatient facilities. Prior to seeking IRB approval, the PI should communicate with the leadership of any ancillary areas that may become involved with the research to ensure the area can commit the necessary resources (e.g. staff, hospital beds, equipment etc.).
Communicating with appropriate areas to ensure resources are available and educating all members of the research team on their roles and responsibilities will help to ensure that the research is implemented in a safe and compliant manner.
Human Subjects Training- Educational Requirements
I completed CITI Training under my affiliation with a former institution. Is that CITI Certificate valid at UConn Health?
CITI Training completed within the last three years may satisfy the UConn Health IRB requirements. However, the IRB reserves the right to require that an individual complete additional modules.
The IRB encourages individuals who are new to UConn Health (e.g. a new student, new faculty member) to complete CITI training under their new affiliation with UConn Health. When completing modules under the new affiliation to UConn Health the CITI Program will provide credit for any overlapping modules completed under another institutional affiliation and will require completion of any modules that are specific to UConn Health requirements.
To affiliate one’s account in the CITI Program with UConn Health, individuals should log into the CITI program, and click on “Add Affiliation” listed under the “Courses” Menu. To find UConn Health in the drop down box, the following words “University of Connecticut” must be typed. Then, select “University of Connecticut Health Center”. To complete the process, check the box next to the statement: “I AGREE to the Terms of Service for accessing CITI Program materials” and check the box with the statement: “I affirm that I am an affiliate of University of Connecticut Heath Center.” Last, click on “Continue.”
To select the correct learning group and courses, follow the “Course Enrollment Questions” posted at https://ovpr.uchc.edu/services/rics/hspp/citi-instructions/
I will be conducting a Clinical Trial at UConn Health. Should I complete the “Good Clinical Practice (GCP)” course?
It depends on whether or not the clinical trial is supported by the National Institutes of Health (NIH). The GCP training is a requirement if the clinical trial is an NIH funded trial. The Human Subjects Protection Program/IRB strongly encourages researches who are involved in clinical research trials not supported by the NIH to complete the GCP course.
Reporting Non-Compliance to the IRB
Principal Investigators are responsible for being knowledgeable of and following the IRB policy for reporting non-compliance (i.e. Policy 2009-002.0.pdf – Reporting Non-Compliance to the Institutional Review Board). Noncompliance is defined in Policy 2011-007.0 as any action that is taken or occurs that is not in accordance with an IRB approved study, IRB polices or regulations or that represents a failure to follow the requirements and/or determinations of the IRB.
Principal investigators (PIs) should report to the IRB any non-compliance that was within the control of the research team within 5 business days of becoming aware of the event. To do so, PIs should complete and submit a Problem Report Form through the IRB online submission system, iRIS. When the non-compliance was not within the control of the research team it should be reported at the time of continuing review. If continuing review is no longer a requirement, non-compliance that was not within the control of the research team should be documented and tracked by the study team and available for review should the study be selected for audit.
Whenever any non-compliance is reported, the investigators should describe the details of the event, the underlying causes of the noncompliance and the actions that have been taken or will be taken to correct the problem and to prevent a subsequent occurrence. PIs should also describe whether the occurrence suggests that subjects or others are placed at an increased risk of harm. This information allows the IRB to accurately assess the situation to determine whether the non-compliance rises to the level of serious and or continuing non-compliance as defined in IRB Policy 2011-007.0 – Definitions Applied to Policies. If the event does rise to the level of serious and/or continuing non-compliance there may be additional reporting required if the research is Federally funded or subject to FDA oversight.
If there is any question about whether reporting is required it is always better to err on the side of caution and report the issue. PI’s are also encouraged to contact one of the Regulatory Specialists to discuss any questions about reporting requirements.
Are you responsible for updating a ClinicalTrials.gov record?
Are you responsible for updating a ClinicalTrials.gov record? You may want to subscribe to the new ClinicalTrials.gov bulletin “Hot off the PRS!” The bulletin details recent updates to the Protocol Registration and Results System (PRS) as well as new resources for PRS users. Enter your email address next to “Receive Updates” at the top of their webpage to subscribe. For help with registering your record or related questions, contact UConn Health’s PRS Administrator, Ellen Ciesielski at 860.679.6004 or eciesielski@uchc.edu.
IRB Forms – Update
The Instructions for Requesting Reliance Upon Advarra IRB.docx have been update to reflect the new contact names at Advarra IRB. Investigators may contact Kathleen Rankin or Ashley Carpenter for guidance in making a submission to Advarra IRB.
Recent Articles Published by Central IRBs
Advarra IRB:
- Gene Therapy: Gene therapy research is at the forefront of a coming boom in the clinical setting. Understand the growth, risks, and regulatory requirements by reading How Centralized IBC Review Can Benefit Gene Therapy Research
- IRB Review of Participant Compensation: IRBs are in charge of reviewing the amount of payment, as well as the method and timing of disbursement, to ensure that the payment plan does not present potential undue influence. Participant compensation is often a complicated matter, what an IRB should consider is discussed at Compensating Clinical Trial Participants: The Basics
Western IRB (WCG):
- Participants Training has a direct impact in achievement the objectives in Clinical trials: Lack of training, particularly for patients, creates variability detrimental to trial findings, says Nathaniel Katz, founder and chief science officer of WCG Analgesic Solutions. To learn more about this topic click on: Lack of Training Compromises Trial Results.
- Recruitment: Recruitment is what drives a study. No patients, no research, right? Sites, sponsors and CROs know they need to do it, but they don’t really consider all the implications or differing strategies to recruitment .To learn more about this topic click on: What You Don’t Know About Patient Recruitment Can Impede the Success of Your Trial
Reporting Race and Ethnicity Data when Requesting Continuing Review
“Researchers assumed that what they learned about white male participants could safely applied to anybody, regardless of gender, race, ethnicity or other variables. We now know that this is not true. When you are communication about research results, it’s vital not only to explain how a study was done, but was being studied,” says Dr. Eliseo J. Perez-Stable, Director of the National Institute on Minority Health and Health Disparities in his article titled: Communicating the Value of Race and Ethnicity in Research.
In August of 2001, The National Institute of Health (NIH) issued a policy which adopted the 1997 Office of Management and Budget (OMB) revised minimum standards for maintaining, collecting, and presenting data on race and ethnicity for all grant applications, contract and intramural proposals and for all active research grants, cooperative agreements, contract and intramural projects. The goal of this policy is to ensure that the distribution of study participants by sex/gender, race and ethnicity reflects the population needed to accomplish the scientific goals of the study.
UConn Health IRB Main Consent Form Template .doc contains an Addendum Form titled “Personal Census Data”. This form provides a mechanism for capturing the representation from racial and ethnic groups in research studies conducted at UConn Health. This addendum form provide instructions to investigators, to present this form to subjects at the time of consent for completion.
The categories and definitions in the “Personal Census Data Sheet” are commonly used for federal data collection purposes. The form’s standards consist of two categories for ethnicity: “Hispanic or Latino” and “Not Hispanic or Latino” and five categories for race: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and White.
Investigator with full board studies or expedited submissions requiring continuing review are required to report this data at the time of request for continuing review.
Investigator should count all subjects who provided consent since the start of the study, including subjects who were screen failures or withdrew. Investigators should indicate by gender the number in each racial/ethnic group. The total reported numbers should equal the total reported since the start of the study in the first table (e.g. first request for continuing review).
The table to be completed within the continuation form in IRIS is provided here for reference.
| Ethnic Category | Females | Males |
| Hispanic or Latino | ||
| Not Hispanic or Latino | ||
| Unknown | ||
| Racial Category | ||
| American Indian/Alaska Native | ||
| Asian | ||
| Native Hawaiian or Other Pacific Islander | ||
| Black or African American | ||
| White | ||
| More Than One Race | ||
| Unknown or Not Reported |
START Preliminary Proof of Concept Fund
Dear Colleagues,
Through a generous grant provided by the CTNext Higher Education Fund last year, the Office of the Vice President for Research (OVPR) has been administering an early stage translational research funding program called the START Preliminary Proof of Concept (PPOC) Fund. Under the grant, funding is provided to investigators at Central Connecticut State University (CCSU), Southern Connecticut State University (SCSU), University of Bridgeport (UB), and UConn on a competitive basis.
The START program aims to support the preliminary validation of innovative early stage technologies that have possible commercial potential and is designed to advance those technologies to be more attractive for additional funding. Proposals for the START PPOC Fund are welcomed from across all disciplines for early stage projects that may one day result in inventions and technologies that address unmet needs and have potential for commercial application.
As we wrap up the first year on funding, I would like to take a moment to recognize recipients from these institutions and ask that you join me in congratulating them on their efforts to commercialize technologies developed in the course of their academic research. For a full list of recipients and project information, visit the OVPR website.
For more information about the competition, visit the program website.
Thank you for helping to foster the culture of excellence in your schools/colleges, departments, and centers that allows UConn faculty to engage in research, scholarship, and creative activities at the highest levels.
Cheers,
Radenka
Celebrating UConn Research, Scholarship, and Creative Activities
Thanks to the tireless work of our faculty, postdocs, students, and staff, our new extramural awards for FY19 reached a three-year high of $266.2M. In FY17, our total new awards were $184.5M and in FY18, they were $258M. UConn Health received over $100M in new awards this past fiscal year reaching an all-time high. Our combined efforts represent a 44% increase over three years. We also saw upward trends in our entrepreneurship and innovation ecosystem, with a record 39 high-potential startup companies joining UConn’s Technology Incubation Program, and a ranking of 93rd worldwide in the number of US patents issued for UConn inventions. It is a matter of great satisfaction for me to have helped position entrepreneurship and innovation as an equal mission for our faculty alongside teaching, scholarship, research and creative work.
Our committed focus on seed funding, proof of concept grants, and awards to support the arts and humanities has contributed to STEM and non-STEM excellence. In FY19, our office contributed $2.3M to internal funding programs and an additional $100K to support grant writing workshops and resources. We are thrilled to see engagement, collaboration, and distinction from all areas of the University, whether it be STEM, non-STEM, or a collaborative hybrid, and that these combined efforts are producing growth in research and extramural awards.
I would like to highlight a few new initiatives launched by the OVPR in FY19 that supported faculty success:
- Convergence Awards for Research in Interdisciplinary Centers (CARIC): Support development of collaborative interdisciplinary teams to bid for major (>$5M) federally funded initiatives, such as research centers.
- Support of UConn Human Rights Institute with two postdoctoral fellowships in collaboration with the Schools of Engineering and Business.
- Program in Accelerated Therapeutics for Healthcare (PATH): In partnership with the Schools of Pharmacy and Medicine, aims to accelerate the translational pathway to convert discoveries into new medical therapeutics. The program seeks to quickly develop novel approaches focusing on well validated molecular targets for a specific disease area with an unmet treatment need in the current commercial marketplace.
- Scholarship and Collaboration in Humanities and Arts Research Program (SCHARP): In partnership with the Humanities Institute, SCHARP supports innovative works in scholarship and creative activities in the arts and humanities that have the potential to transform a field of study, impact the common good, or chart a new direction in scholarly, creative, or artistic direction.
- STEAM Innovation Grant: In partnership with the School of Fine Arts, STEAM encourages innovative collaborations between the arts and STEM disciplines. Projects funded by this grant may result in publications, exhibitions, performances, academic symposia, or other research outcomes.
- Stamford Innovate, a new internship program that connects talented UConn students with opportunities in startups in one of the fastest growing regions of the state.
If you want to learn more, click here for a full list of our internal funding programs.
As educators, we all take great pride in our students’ successes, and I wanted to take a moment to recognize some new student projects that are truly remarkable. In collaboration with the Office of the Provost, the OVPR supported a student-led podcast called In Vivo. With regular interviews about science, the arts, current events, and other topics, In Vivo highlights the amazing faculty, students, and staff that give UConn life. The show is conducted out of UConn’s WHUS studio and is run entirely by UConn students. Check it out and consider subscribing for future episodes to learn more about UConn researchers.
Another new initiative is World Poetry Books to support its mission of publishing and vigorously promoting a minimum of six books of exceptional poetry in translation each year. This support offers our students the opportunity to gain hands-on, professional publishing skills, and establishes UConn as home of a preeminent publisher of exceptional world literature.
While sharing accomplishments is important, we also want to increase transparency and continue to maintain open lines of communication as we push to raise UConn’s research profile. In addition to sharing research and tech transfer metrics on the recently revamped UConn Research website, we encourage faculty and staff to reach out with suggestions regarding new opportunities and unmet needs. It is only together – as a team – that we will continue to drive the growth of scholarship, research, and creative pursuits at UConn.
I’d like to conclude with a personal note of gratitude. I cannot thank all of you enough for giving me the opportunity to work with so many talented, hardworking, and committed colleagues. To my staff, I am deeply honored to serve as VPR and grateful for your support, continued improvement, and service to our faculty and students. At the end of a hard day, I find great inspiration in the knowledge that UConn’s faculty and staff – whether they be musicians, chemists, or scholars of law or other disciplines – are some of the world’s most innovative and active researchers. Thank you for making UConn a special place with a vibrant community of caring, collaborative people.
We are opening a new chapter for UConn with a new President who is focused on our excellence, strengths, and new opportunities. I look forward to this journey with all of you, and please remember my door is always open!
Cheers,
Dr. Radenka Maric
Vice President for Research, UConn/UConn Health
Prospective Basic Science Studies Involving Human Participants
On July 24th, NIH published a Guide Notice (NOT-OD-19-126) announcing the extension of delayed enforcement of registering and results reporting of Basic Experimental Studies involving Humans (BESH trials) on ClinicalTrials.gov through September 24, 2021. BESH trials are basic research projects exploring fundamental aspects of phenomena that involve human participants.
In a previous RFI (NOT-OD-18-217), NIH solicited feedback from the scientific community about challenges in reporting BESH trials on the ClinicalTrials.gov platform and several primary challenges were identified. Therefore, NIH has determined that more time is needed to address these challenges. In the interim, to meet NIH’s registration and results reporting requirement, alternative publicly available platforms should be used as described at the time of application in the Dissemination Plan attachment.
Please note this extension does not change the requirement for clinical trials to be registered on ClinicalTrials.gov.
For questions about this notice or your ClinicalTrials.gov requirement, please contact Ellen Ciesielski, 860.679.6004.
Important Information from the NIH and NSF
Dear Investigator,
On July 10th, the National Institutes of Health (NIH) published a reminder on NIH Policies on Other Support and on Policies related to Financial Conflicts of Interest and Foreign Components. This was followed on July 11th by a Dear Colleague Letter on protecting research funded by the National Science Foundation (NSF) from NSF Director, Dr. France Córdova. These notices relate to the ongoing concerns regarding foreign influence in federally funded research.
In response to these publications, the OVPR recommends that any collaborations with foreign entities or individuals, or appointments with foreign entities (including foreign talent or similar programs) be disclosed to the NIH or NSF program officer, your Dean, and the OVPR (contacts and additional information listed below).
The OVPR has posted additional guidance on our site regarding Active and Pending Support and Foreign Collaborations. For any questions or for guidance on this and other related matters, please contact:
- Laura Kozma, Executive Director SPS (laura.kozma@uconn.edu)
- Paul Hudobenko, Director SPS – UConn Health (hudobenko@uchc.edu)
Thank you for your cooperation,
Radenka Maric, PhD
Vice President for Research
UConn/UConn Health
Important Information from the NIH and NSF for UConn/UConn Health Investigators
The NSF Letter references the draft NSF Proposal and Award Policies & Procedures Guide published in May 2019. Clarifications in the draft Guide related to current and pending support and biographical sketches include:
- Providing information for all current and pending support irrespective of whether such support is provided through the proposing organization or directly to the individual.
- Expanding examples of current and pending support to include non-profit organizations and consulting agreements.
- Reporting all projects and activities requiring a time commitment (no minimum has been established), even if the support received is only in-kind.
- Appointments should include any titled academic, professional, or institutional position whether or not remuneration is received.
The Dear Colleague Letter also states the NSF will be issuing a policy that NSF personnel and Intergovernmental Personnel Act (IPA) assigned personnel cannot participate in foreign government talent-recruitment programs.
The NIH Notice reminds applicants that in regards to Other Support, they must:
- List all positions and scientific appointments, both domestic and foreign, held by senior/key personnel which are relevant to an application including affiliations with foreign entities or governments such as titled academic, professional, or institutional appointments whether or not remuneration is received, and whether full-time, part-time, or voluntary (including adjunct, visiting, or honorary).
- Report all resources and other support for all individuals designated in an application as senior/key personnel – including the program director/principal investigator and other individuals who contribute to the scientific development or execution of a project in a substantive, measurable way, whether or not they request salaries or compensation. All current support for ongoing projects must be included, irrespective of whether such support is provided through the applicant organization, through another domestic or foreign organization, or is provided directly to an individual who supports the senior/key personnel’s research efforts.
- Report all current projects and activities involving senior/key personnel, even if the support received is only in-kind (e.g. office/laboratory space, equipment, supplies, employees), including, but not limited to, foreign financial support, research or laboratory personnel, lab space, scientific materials, selection to a foreign “talents” or similar-type program, or other foreign or domestic support.
- Provide the total award amount for the entire award period covered (including facilities and administrative costs), as well as the number of person-months (or partial person-months) per year to be devoted to the project by the senior/key personnel.
The Notice also reminds applicants of the need to determine whether projects include a foreign component, defined as the existence of any “significant scientific element or segment of a project” outside of the United States including:
- Performance of work by a researcher or recipient in a foreign location, whether or not NIH grant funds are expended and/or
- Performance of work by a researcher in a foreign location employed or paid for by a foreign organization, whether or not NIH grant funds are expended.
If a significant portion of a project will be conducted outside the United States, then there is a foreign component and NIH prior approval is required. If all project activity is conducted within the United States, but there is a non-U.S. resource supporting the project, it must be reported as other support.
HSPP-April-May-June,2019 -Newsletter
UConn Health’s Human Subjects Protection Program Receives Reaccreditation from the Association for the Accreditation of Human Research Protection Programs (AAHRPP)
The Association for Accreditation of Human Research Protection Programs (AAHRPP) completed a site visit at UConn Health in April 2019. During this visit, IRB members and staff, investigators and study coordinators, and others involved with research oversight were interviewed, and study research records were reviewed. In June 2019, the AAHRPP Council on Accreditation awarded full reaccreditation to UConn Health’s Human Subjects Protection Program (HSPP), confirming that all standards for re-accreditation were fulfilled. This reaccreditation is for five additional years. The final report issued by AAHRPP commends the HSPP for demonstrating an unusually high degree of integration among the areas responsible for research oversight.
Documentation of Consent
Unless the requirement to document consent has been waived by the IRB, the IRB approved consent form must be signed and dated by the subject (or legally authorized representative) and the person obtaining consent.
Notes in a research chart that indicate on-going discussions with the subject at subsequent study visits may supplement documentation of the initial informed consent process.
The following are examples of issues found with documentation of consent during recent internal audits at UConn Health.
- The date of consent differs between the subject and the person obtaining consent.
- The date of consent is left blank by the subject and/or the person obtaining consent..
- The date of signature is incomplete or incorrect.
- The informed consent form is missing the signature of the person obtaining consent.
- The person obtaining consent enters the date of the subject’s signature.
- Consent for participation obtained from legally authorized representatives when the study approval requires the subject to provide consent.
- Consent was obtained by people not approved as consenters by the IRB.
- Subjects consented with expired consent documents.
- Consent forms containing a correction to the signature and/or date which obscured the original entry.
To ensure consent is appropriately documented the following points should be considered:
- The principal investigator and study team members should use the most recently approved stamped and dated consent form when obtaining consent.
- Subjects should sign the consent form in the presence of, and at the same time as, the consenter.
- Persons obtaining informed consent should review the forms once they are signed/completed and before the subject leaves that day, to ensure that all signatures and dates are properly entered on the forms.
- In the event that a form is found to be incomplete (e.g., a date is missing) if the error is not discovered while the subject is present, the research staff should prepare a note to file attesting to the fact that they witnessed the signing of the form, and the date that it was signed. The original consent form must be retained, and the subject should make the corrections at the earliest opportunity.
- Any problem with documentation of informed consent should be reported to the IRB using a problem report form within five days of becoming aware of the non-compliance.
- Approved consenters should review HSPP Policy 2011-008.1.pdf – Informed Consent – Process and Policy 2011-008.5.pdf – Informed Consent – Providing and Obtaining Informed Consent
Guidance for Posting Clinical Trial Consent Forms
Last January 2019, the revised version of 45 CFR 46, the federal regulation for the protection of human subjects in research, which is also known as the Common Rule, went into effect. One of the revisions requires that for any clinical trial conducted or supported by a Common Rule department or agency, one IRB-approved consent form that was used to enroll subjects be posted on a publicly available federal website within a specific time frame. UConn Health IRB has posted a Guidance for Posting Clinical Trial Consent Forms to help the research community to fulfill this obligation.
IRB Forms – Update
Investigators should always use the latest version of the IRB forms posted in the IRB website. Listed below, are the forms revised during the past three months. Within the parenthesis is the date when forms were revised.
- Instructions for Requesting Reliance Upon Advarra IRB.docx (4/24/2019 – template consent language updated per Advarra requirement)
- Confirmation of Resources for Inpatient Stays.docx (4/25/2019 – added comment section in sign-off area)
- Request for Full or Partial Waiver Informed Consent.doc (4/25/2019 – added note that approval of waiver not applicable to information/samples if original consent stated there would be no future use of information/samples)
- Application Appendix A.doc (CRC Resource Request) (5/21/2019 by CRC)
- Application Checklist for Initial and Continuing Review Full Board.docx (6/25/2019 – changed pharmacy contact)
- Application Checklist for Initial Exempt Application .doc(5/1/2019 – removed CICATS references)
- Application Checklist for Initial and Continuing Review Expedited .doc (6/25/2019 – changed pharmacy contact)
- Application Checklist to Request Facilitated Review for Industry or Cooperative Group Sponsored Study, or study utilizing the SMART IRB Initiative.docx (6/25/2019 – changed pharmacy contact)
- Main Consent Form Template .doc (6/12/2019 – changed reference Health One to EPIC, added reminder about mobile device security, rather than instructional text/samples about when FDA/DHHS/Sponsor can inspect records changed to “as may be applicable” and reference all three.)
- HIPAA Authorization to Use and Disclose.doc (6/28/2019 – deleted instructional text at top of form)
- HIPAA Authorization to Use and Disclose – Spanish.doc 6/28/2019 )
Personnel Changes to the Scientific Review Committee
Dr. Doug Peterson who has served as the Chair of the Scientific Review Committee (SRC) for over a decade has stepped down as Chair. Dr. Julie Wagner is now the SRC Chair and Dr. Peterson will continue to serve on the SRC as a member until November 1.
The following three faculty members have been appointed to serve on the SRC.
- Dr. Efthimia Ioannidou, Professor/Clinical, Periodontology
- Dr. Ivo Kalajzic, Professor/Basic Science, Center for Regenerative Medicine
- Dr. Tannin Schmidt, Associate Professor/Basic Science, BioMedical Engineering
In Memoriam – Pamela Engelson Colwell
Our dear friend and colleague, Pamela E. Colwell (Pam) passed away on Wednesday, June 26, 2019. Pam worked for the IRB for the last 15 years as a Regulatory Specialist and IRB member. Pam was an amazing team member, taught multiple IRB members, and played a pivotal role in the implementation of the iRIS submission system. Please refer to the following link for information regarding services and memorial donations. http://northhavenfuneral.com/obituary/pamela-engelson-colwell/
UConn Health’s Human Subjects Protection Program Receives Reaccreditation from AAHRPP
Dear Colleagues,
It is my pleasure to inform you that we received official notification from the Association for the Accreditation of Human Research Protection Programs (AAHRPP) of continuing Full Accreditation for the UConn Health Human Subjects Protection Program. The process to obtain reaccreditation is an important, but complex one, which required team work from many stakeholders. I would like to take this opportunity to thank faculty and staff, IRB members and staff of the HSPP, members of the Scientific Review and Conflicts of Interest committees, Office of Clinical and Translational Research Services, Sponsored Program Services, Research Pharmacy and Research Safety, and many others who are committed to ensuring that we have an outstanding human subjects program every day. They are to be commended for their dedication and efforts in maintaining our continued accreditation. Their work ensures appropriate care of clinical trial participants, which in turn makes possible the high quality research conducted by UConn Health investigators.
Sincerely,
Wesley G. Byerly, Pharm.D.
Associate Vice President
Program in Accelerated Therapeutics for Healthcare (PATH) Awards
Dear Colleagues,
I’m very pleased to announce that the Office of the Vice President for Research (OVPR) has recently finalized award decisions for the inaugural cycle of the Program in Accelerated Therapeutics for Healthcare (PATH). PATH is a partnership that includes the OVPR, the School of Pharmacy, and the School of Medicine to accelerate the translational pathway for researchers to convert their discoveries to new medical therapeutics. Under PATH, funding is provided to academic research programs designed to quickly develop novel therapeutic approaches focusing on well validated molecular targets for a specific disease area with an unmet treatment need in the current commercial marketplace. Projects focusing on a wide range of therapeutic interventions (small molecule, biologic, antibody, peptide, gene therapy) are eligible for consideration.
Given your leadership role in the University, I want you to be among the first to hear the results of this competition so you can join me in congratulating the awardees. Seven PATH grants were awarded in two categories after a highly selective competition:
PATH Trailblazer Grants – $75,000
Xiuling Lu, Pharmaceutical Science
Cutting Cancer at Its Root: Inhibition of Acute Leukemic Stem Cells Using Doxorubicin-Loaded Nanoparticles
Jessica Rouge, Chemistry
Determining the Pharmacology of a Novel DNAzyme-therapeutic Formulation for the Treatment of Allergic Airway Disease
PATH Ascent Grants – $10,000
Brian Aneskievich, Pharmaceutical Science
Establishing Protein Conformational Flexibility to Enhance Next-Step Drug-Screen Targeting
Nicholas Leadbeater, Chemistry
Towards Development of Novel Therapeutics for Treatment of Toxoplasmosis
Rajkumar Verma, Neuroscience, UConn Health
Discovery of Novel Purinergic P2X4 Receptor Antagonist for the Treatment of Ischemic Stroke
Simon White, Molecular and Cell Biology
Screening for Small Molecule Inhibitors against Enterovirus D68 2C Helicase
Ming Xu, Genetics and Genome Sciences, UConn Health
Discover Drugs Targeting Cellular Senescence to Improve Healthspan and Lifespan
For more information about PATH, visit the program website.
Thank you for helping to foster the culture of excellence in your schools/colleges, departments, and centers, that allows UConn faculty to engage in research, scholarship, and creative activities at the highest levels.
Cheers,
Radenka
OVPR Quarterly Reports – FY19Q2
Dear Colleagues,
Now that data have been finalized, I would like to provide you with several reports relating to sponsored program activity—both research and education/service—managed by Sponsored Program Services within the Office of the Vice President for Research at UConn and UConn Health. Please visit the OVPR website to view the following reports: https://research.uconn.edu/reports/reports-archive/
- List of Proposals Submitted: FY19 2nd Quarter
- List of Awards Received: FY19 2nd Quarter
- Proposals, Awards, Expenditures: FY14-FY19Q2
In the reports, data are presented in two ways: by the PI’s Academic Home Department and by the Managing Department or Center/Institute. Please refer to the first pages of the reports for definitions and information regarding the data. Should you have any questions regarding these quarterly reports, please do not hesitate to contact me.
Please note that we have included an additional Summary of Sponsored Program Activity, which includes the Effective F&A rate on awards. This information provides a snapshot of our activity as compared to the same period last year.
The OVPR continues to seek creative solutions that allow UConn and UConn Health to grow our research enterprise through federal funding, industry partnerships, and collaboration with foundations. I am confident we can continue upward trends by continuing to work together, aggressively applying for extramural funding, and pursuing new channels of support for the tremendous research, scholarship, and creative activities taking place every day at UConn and UConn Health.
Thank you for your continued commitment and contribution to our students, to your research and scholarship, and to UConn/UConn Health.
Sincerely,
Radenka
Dr. Radenka Maric
Vice President for Research
UConn/UCH
HSPP- Jan-Feb-Mar, 2019 – Newsletter
Revised Common Rule (45 CFR 46)
The revised version of the regulation governing human subjects research (i.e. 45 CFR 46 also known as the Common Rule) became effective January 21, 2019. Due to this revision, several IRB forms, templates, and policies have been modified. Always refer to the HSPP web site to ensure you are using the most recent version of a form.
The following sections contain a summary of those changes.
-
- The Consent Form Template and Consent Checklist were revised to incorporate seven new elements of consent for federally funded/supported research. For those approved federally funded/supported research studies that are actively enrolling subjects, investigators should submit either at the time of continuation or through a request for modification a revised consent form with the new required elements. Until such time as this review occurs studies are considered grandfathered under the current version of the Common Rule. Subjects will not be required to be re-consented based solely on these changes. For federally funded/supported studies that are closed to new enrollment the consent form will need to be revised only if there is another reason that triggers a change to the document. For example if new risks are being disclosed, at the time the consent is revised to incorporate the new risk the consent would also have to be brought into compliance with the new requirements. For previously approved non-federally funded/supported research, no changes are necessary; however, these new elements will be used as the guiding principle of consent elements moving forward.
- Waiver/Alteration of Consent: If the research involves using identifiable private information or identifiable biospecimens, the investigator will need to explain in the waiver document why the research could not practicably be conducted without access to and use of the identifiable private information/biospecimens.If a waiver is necessary for federally funded/supported studies investigators must be sure to address the additional element describe above at the time the study is transitioned to the revised rule. Waiver of Documentation of Consent: There is a new provision for allowing for waiver of documentation of consent. Documentation of consent may also be waived if the subjects or legally authorized representatives are members of a distinct cultural group or community in which signing forms is not the norm, that the research presents no more than minimal risk of harm to subjects and provided there is an appropriate alternative mechanism for documenting that informed consent was obtained.
- Changes to Continuing Review Requirement: Unless otherwise required and justified by the IRB, continuing review will no longer be required for non-FDA regulated federally funded research that meets the criteria for expedited review. Investigators who have non-FDA regulated federally funded research that qualifies for expedited review will be asked to provide an expected completion date of the research, which will become the expiration date of IRB approval. For previously approved research this may be provided as part of one last request for continuation (e.g. if IRIS has already generated a continuing review due task) or as part of a request for modification. The PI will be required to submit a request for modification to extend this expected completion date if necessary. The IRB may require justification for the expected completion date as it deems appropriate. Note: Continuing review is still a requirement for all FDA regulated research even if all subjects are in long-term follow-up or the research is in data analysis.
Any study that does not requires continuing review still need to submit a modification to the IRB prior to implementing changes to the conduct of that study except when the change is necessary to eliminate immediate hazards to subjects. Modifications include, but are not limited to, change in design, removal or change to survey tool, change in funding source, change to recruitment materials, adding or removing investigators, changing the title of the project, requesting additional subjects beyond the original approved number, changes to informed consent forms, or other correspondence with potential or current subjects.
4. Changes to the Initial Application Form in IRIS: The IRB application form in IRIS was edited. The request for Exempt status categories and Expedited review categories were removed from the application and are now described in two separate word documents to be attached to the application form in IRIS. The following forms have been published in the IRB website and should be submitted when requesting a determination for exemption or review under an of the expedited categories:
5.The following IRB forms have been updated and published in the IRB website:
-
- Checklist for Initial and Continuing Review Expedited .doc
- updated to reference the request for expedited review form
- Checklist for Initial Exempt Application .doc
- (updated to reference the request for exemption form
- Consent Checklist – Addendum to Transition to Revised Common Rule.doc
- created to list only new elements of 45 CFR 46 to incorporate into previously approved consent forms
- Human Subject Research Determination Form.doc
- based on updated definitions and activities that are deemed not to be research
Points to Remember When Relying on an External IRB
- With the exception of reporting changes in study personnel, once the determination is made to accept the external IRB as the IRB of Record, from that point forward the UConn Health investigator only deals with the IRB of Record for the review of continuations, modifications, unanticipated problems and non-compliance.
- The Principal Investigator is responsible for knowing and following the requirements of the reviewing IRB, inclusive of requirements for reporting subject complaints, non-compliance, unanticipated problems and outcomes of audits and inspections. The PI is responsible for ensure that the research team is also aware of and follows such.
- Research for which IRB oversight has been deferred to an external IRB may still be subject to audit by the UConn Health Research Compliance Monitor.
Difference between Privacy and Confidentiality
Privacy applies to the individual and confidentiality applies to the data obtained from the individual.
According to the IRB Guidebook, published by the Office for Human Research Protections (OHRP 1993): “Privacy can be defined in terms of having control over the extent, timing, and circumstances of sharing oneself (physically, behaviorally, or intellectually) with others. Confidentiality pertains to the treatment of information that an individual has disclosed in a relationship of trust and with the expectation that it will not be divulged to others, in ways that are inconsistent with the understanding of the original disclosure without permission.”
Therefore, the privacy of the subjects in a research study can be maintained by conducting the consent process, interviews, and procedures in a private room. The confidentiality of the subjects’ data can be protected, for example, by storing the data on encrypted password protected computers.
Expanded Definition of “Clinical Trial” & ClinicalTrials.gov
The Revised Common Rule expanded the definition of “clinical trial” with the intention of harmonizing with the National Institutes of Health’s definition. The expanded definition includes any “research study in which one or more human subjects are prospectively assigned to one or more interventions (which may include placebo or other control) to evaluate the effects of those interventions on biomedical or behavioral health-related outcomes.” Importantly, the revised definition includes studies that had not previously been considered clinical trials, like social and behavioral research.
What if my study meets the expanded definition of a clinical trial?
1) If your clinical trial is funded by a Federal department or agency, the Revised Common Rule requires that your consent form be posted on a public platform, like ClinicalTrials.gov, after the trial is closed to recruitment, and no later than 60 days after the last subject visit.
2) If your clinical trial evaluates at least one drug, biological, or device product regulated by the FDA (See this decision checklist for more details), regardless of funder, you are required to register and post results on ClinicalTrials.gov.
3) If your clinical trial is NIH funded, in whole or in part, you are required to register the study and report results on ClinicalTrials.gov.
4) Regardless of funder, if you wish to comply with the ICMJE policy (followed by the BMJ, JAMA and many other journals) requiring registration as a condition of consideration for publication, you may voluntarily register your study with ClinicalTrials.gov.
For assistance with ClinicalTrials.gov, see our webpages and contact UConn Health’s ClinicalTrials.gov Administrator, Ellen Ciesielski (860-679-6004) in Research Integrity and Compliance Services.
2019 CARIC Award Recipients Announced
Dear Colleagues,
I am pleased to announce that two teams have been selected for funding in the inaugural cycle of CARIC (Convergence Awards for Research in Interdisciplinary Centers).
CARIC supports the development of collaborative, interdisciplinary teams bidding for major federally funded research initiatives. These initiatives can include large, multi-million-dollar research grants or even entire research centers.
2019 CARIC Awards:
- David Rowe, Director of the Center for Regenerative Medicine and Skeletal Development
Bed to Bench (BTB) Collaboration for Skeletal Research - Yu Lei, Castleman Distinguished Professor, Chemical and Biomolecular Engineering
Exposure, Health Effects, Sensing and Remediation of Emerging Contaminants Superfund Research Program (SRP) Center
The CARIC program will provide these projects with funding of up to $150,000 to support planning, outreach to strategic partners and proof-of-concept research for a year, with the possibility for renewal. This initial funding allows researchers to develop more competitive bids for prestigious national awards.
To learn more about CARIC, visit the website of the Office of the Vice President for Research.
Sincerely,
Dr. Radenka Maric
Vice President for Research
UConn/UConn Health
HSPP- October-November-December, 2018
Overview of Major Changes to the Common Rule (45 CFR 46)
The revised version of the regulation governing human subjects research (i.e. 45 CFR 46 also known as the Common Rule) became effective January 21, 2019. Accordingly, several IRB forms, documents templates, policies and the IRB applications in IRIS have been revised. It is the intention of the IRB that all federally funded/supported research will be brought into compliance with the revised regulation at the time of the continuing review that occurs on or after January 21, 2019. Until such time as that review occurs those studies are considered grandfathered under the previous version of the regulation. Investigators may request to transition to the revised regulation soon by submitting a request for modification.
The following sections contain a summary of the major changes.
The Consent Form Template and Consent Checklist have been revised to incorporate seven new elements of consent for federally funded/supported research. The new requirement regarding process and the new 7 elements of a consent are as follows
- Consent must begin with a concise and focused presentation of the key information that is most likely to assist a prospective subject or LAR in understanding the reasons why one might or might not want to participate in the research. This part of the informed consent must be organized and presented in a way that facilitates comprehension
- Informed consent as a whole presents information in sufficient detail relating to the research, and is to be organized and presented in a way that does not merely provide lists of isolated facts, but rather facilitates the prospective subject’s or LAR’s understanding of the reasons why one might or might not want to participate
- One of the following statements if the research involves the collection of identifiable private information (IPI) or identifiable biospecimens (IB):
- A statement that identifiers might be removed from the IPI or IB and that, after such removal, the information or biospecimens could be used for future research studies or distributed to another investigator for future research studies without additional informed consent from the subject or the LAR, if this might be a possibility; OR
- A statement that the subject’s information or biospecimens collected as part of the research, even if identifiers are removed, will not be used or distributed for future research studies
- If applicable, a statement that the subject’s biospecimens (even if identifiers are removed) may be used for commercial profit and whether the subject will or will not share in this commercial profit
- If applicable, a statement regarding whether clinically relevant research results, including individual research results, will be disclosed to subjects, and if so, under what conditions
- If applicable, for research involving biospecimens, whether the research will (if known) or might include whole genome sequencing (i.e. sequencing of a human germline or somatic specimen with the intent to generate the genome or exome sequence of that specimen).
For those approved federally funded/supported research studies that are actively enrolling subjects, investigators should submit either at the time of continuation or through a request for modification a revised consent form with the new required elements. Until such time as this review occurs studies are considered grandfathered under the current version of the Common Rule. Subjects will not be required to be re-consented based solely on these changes.
For federally funded/supported studies that are closed to new enrollment the consent form will need to be revised only if there is another reason that triggers a change to the document. For example if new risks are being disclosed, at the time the consent is revised to incorporate the new risk the consent would also have to be brought into compliance with the new requirements.
For previously approved non-federally funded/supported research, no changes are necessary; however, these new elements will be used as the guiding principle of consent elements moving forward.
To learn more about the new elements of consent please review IRB Policy 2011-008.0.pdf– Informed Consent – Forms
The revised regulation expands the definition of Legally Authorized Representative to now recognize that if State law is silent legally authorized representative means an individual recognized by institutional policy as acceptable for providing consent in the non-research context on behalf of the prospective subject to the subject’s participation in the procedure(s) involved in the research.
To learn more about the new changes to the consent process please review IRB Policy 2011-008.5.pdf – Informed Consent – Providing and Obtaining Informed Consent
Waiver/Alteration of Consent: When a waiver or alteration of consent is requested the following additional criterion must be met in order for the IRB to grant the waiver/alteration.
- If the research involves using identifiable private information or identifiable biospecimens, the research could not practicably be carried out without using such information or biospecimens in an identifiable format.
If a waiver is still necessary (see below) for federally funded/supported studies investigators must be sure to address this additional element at the time the study is transitioned to the revised rule.
The revised regulation allows for certain activities regarding screening, recruiting or determining eligibility (e.g. telephone screening or chart reviews for the purpose of determining eligibility) to occur without a waiver/alteration if either of the following conditions are met:
- The investigator will obtain information through oral or written communication with the prospective subject or legally authorized representative, or
- The investigator will obtain identifiable private information or identifiable biospecimens by accessing records or stored identifiable biospecimens.
The above change has been already be implemented for non-federal studies, and as of January 21, 2019 will be implemented to federally funded studies. If a waiver had been previously approved but is no longer necessary, that document should not be included in the submission packet at the time the study is transitioned to the revised rule.
Note: There has been no change to HIPAA and there must be adequate measures in place to protect the confidentiality of any information collected for the purpose of screening, recruiting or determining eligibility prior to informed consent.
To learn more about the new changes to the waiver of consent please review IRB Policy 2011-008.2.pdf – Informed Consent – Waivers and Alterations
Waiver of Documentation of Consent: There is a new provision for allowing for waiver of documentation of consent. Documentation of consent may also be waived if the subjects or LAR are members of a distinct cultural group or community in which signing forms is not the norm, that the research presents no more than minimal risk of harm to subjects and provided there is an appropriate alternative mechanism for documenting that informed consent was obtained.
To learn more about the new changes to the waiver of documentation of consent please review IRB Policy 2011-008.2.pdf – Informed Consent – Waivers and Alterations
Changes to Continuing Review Requirement: Unless otherwise required and justified by the IRB, continuing review will no longer be required for non-FDA regulated federally funded research that meets the criteria for expedited review.
Investigators who have non-FDA regulated federally funded research that qualifies for expedited review will be asked to provide an expected completion date of the research, which will become the expiration date of IRB approval. For previously approved research this may be provided as part of one last request for continuation (e.g. if IRIS has already generated a continuing review due task) or as part of a request for modification. The PI will be required to submit a request for modification to extend this expected completion date if necessary. The IRB may require justification for the expected completion date as it deems appropriate.
Note: Continuing review is still a requirement for all FDA regulated research even if all subjects are in long-term follow-up or the research is in data analysis. The IRB has already implemented this practice for expedited research that is not federally funded or subject to FDA oversight.
New Exempt Categories : There have been several revisions to the types of research that may be exempt and the exemptions may now apply to research that only incidentally includes prisoners as subjects (e.g. the research is aimed at involving a broader subject population and only incidentally includes a subject who became incarcerated after providing consent). These categories are applicable regardless of funding source. The new exemption categories are described in the form titled Request for Exemption
Any study previously granted an exemption remains grandfathered under that exemption.
Studies that had been approved through the expedited process that may qualify for exemption under the revised regulation will be transitioned to exempt status on a case-by-case basis as requests for continuation or modifications are received.
To learn more about the revised Exempt categories please review Policy # 2011-009.2.pdf – Institutional Review Board – Exemptions
Changes to the Initial Application Form in IRIS: The IRB application form in IRIS has been edited. The request for Exempt status categories and Expedited review categories have been removed from the application and are now described in two separate word documents to be attached to the application form in IRIS. The following forms have been published in the IRB website:
- The following IRB forms have been updated and published in the IRB website:
- Application Checklist for Expedited Review (to reference request for expedited review form)
- Application Checklist for Exemption (to reference request for exemption form)
- Consent Checklist Addendum to Transition to Revised Rule (lists only new elements of 45 CFR 46 to incorporate into prior version of ICF for studies approved prior to 1/21/2019)
- Human Subject Determination Form (based on updated definitions and activities that are deemed not to be research)
RESEARCHMATCH NOW AVAILABLE IN SPANISH!
ResearchMatch (RM) is the national online recruitment tool that matches people interested in participating in studies with researchers throughout the U.S. There is no cost to UConn Health researchers to use ResearchMatch. Once you register as a researcher, you can review the population characteristics of the ResearchMatch registry, which includes over 135,000 people from every state in the country.
*NEW* ResearchMatch has just launched a Spanish version of the website inviting Spanish speakers to sign up in Spanish. Researchers from UConn Health are now able to connect with and recruit Spanish-speaking volunteers for their studies.
If you would like to use ResearchMatch, you will need IRB approval for this recruitment method, including approval of the contact message emailed to volunteers. ResearchMatch can be added to an already-approved study via a modification.
Interested in using ResearchMatch? Sign up now, attend an online training, or visit our webpage or contact Ellen Ciesielski for more information.
Already registered with ResearchMatch and want to recruit Spanish-speaking volunteers? Submit your ResearchMatch contact message and other materials translated into Spanish (consent form, questionnaires, etc.) for IRB approval and ensure you are prepared for inquiries from Spanish-speaking volunteers.
OVPR Quarterly Reports – FY19Q1
Dear Colleagues,
Now that data have been finalized, I would like to provide you with several reports relating to sponsored program activity—both research and education/service—managed by Sponsored Program Services within the Office of the Vice President for Research at UConn and UConn Health. Please visit the OVPR website to view the following reports:
- List of Proposals Submitted: FY19 1st Quarter
- List of Awards Received: FY19 1st Quarter
- Proposals, Awards, Expenditures: FY14-FY19Q1
In the reports, data are presented in two ways: by the PI’s Academic Home Department and by the Managing Department or Center/Institute. Please refer to the first pages of the reports for definitions and information regarding the data. Should you have any questions regarding these quarterly reports, please do not hesitate to contact me.
Please note that we have included an additional Summary of Sponsored Program Activity, which includes the Effective F&A rate on awards. This information provides a snapshot of our activity as compared to the same period last year.
The OVPR continues to seek creative solutions that allow UConn and UConn Health to grow our research enterprise through federal funding, industry partnerships, and collaboration with foundations. I am confident we can continue upward trends by continuing to work together, aggressively applying for extramural funding, and pursuing new channels of support for the tremendous research, scholarship, and creative activities taking place every day at UConn and UConn Health.
Thank you for your continued commitment and contribution to our students, to your research and scholarship, and to UConn/UConn Health.
Sincerely,
Radenka
Sponsored Program Guidance during the Partial Federal Government Shutdown
Updated: 12/27/2018 with additional agency specific guidance and information.
Effective Saturday, December 22nd at 12:00am, appropriations for fiscal year 2019 for approximately 25% of the federal government expired. Agencies who have full appropriations and are not currently impacted by the partial shutdown include Veterans Affairs, Department of Defense and Department of Health and Human Services (including NIH). Agencies that are impacted by the partial shutdown include the National Science Foundation, Department of Agriculture, Department of Transportation, Department of State, Department of Justice and NASA.
Interim guidance for agencies impacted by the partial shutdown is provided below. Additional guidance will be provided if the shutdown persists. If you have specific questions about a proposal or award, please contact Sponsored Program Services.
Proposals
- If the electronic system for submission is operating, the proposal should be submitted by the deadline in the solicitation in accordance with standard practice.
- If the electronic system for submission is not operational or offline, the proposal will not be submitted until further guidance is received from the federal sponsor. To be safe, SPS recommends that you prepare your proposal for submission as best you can by the published deadline, even if it cannot be submitted.
- Currently Grants.gov and FastLane (NSF submissions) is available and operational.
Award Management
- Current funded awards may continue regular activities and incur normal expenses (exception: NSF payments systems are not operational – contingency plans will need to be further discussed if the shutdown persists longer than a couple weeks).
- Contact SPS prior to charging any major or capital expenses.
- UConn may not receive new awards during the shutdown.
- Sponsor required prior approval requests (i.e. No Cost Extension requests) may not be approved during the shutdown.
- Please contact SPS with specific questions about your award.
Agency Specific Guidance during the Shutdown
NSF
https://www.nsf.gov/shutdown/grantees.jsp
- No new funding opportunities will be issued.
- FastLane and Research.gov is available for most functions but NSF will not process proposals or prior approval requests until normal operations resume.
- Annual and final project reports should be submitted by the due date however they will not be processed and continuing grant increments will not be issued.
- No new grants or cooperative agreements will be awarded.
- No prior approvals and no payments will be made during the shutdown.
Additional Agency Specific Guidance and Information
UPDATE: Partial Federal Government Shutdown, 12/27/18
NASA
If your grant or cooperative agreement requires access to a NASA facility or participation from NASA personnel in order to perform the instrument’s stated research objectives, the guidance in paragraph (a) below is applicable. If your grant or cooperative agreement does not require access to a NASA facility or participation of NASA personnel in order to perform the instrument’s stated research objectives, the guidance in paragraph (b) below is applicable.
-
- To the extent the grant or cooperative agreement includes work performed on-site at a NASA facility, the NASA facility will not be available for the performance of such work beginning on December 26, 2018. You are instructed to commence an orderly shut-down of your onsite operations and you are to preserve resources and take all actions necessary to minimize costs incurred under the subject grant or cooperative agreement during this Government shutdown. This includes notifying your employees immediately of this orderly shutdown. Contact Sponsored Program Services immediately if this applies to your award.
- Since your grant or cooperative agreement does not require access to a NASA installation, access to NASA IT resources and data, or participation of NASA personnel in order to perform the instrument’s stated research objectives, you are to continue to perform research under your grant or cooperative agreement as long you have available funding. Special Condition 1260.53 Incremental Funding (for awards subject to 14 CFR Part 1260) or Term and Condition 1800.921 Incremental Funding (for awards subject to 2 CFR Part 1800) of your grant or cooperative agreement specifies the total amount of funding that has been allotted to your grant or cooperative agreement. You are also reminded the Agency is not obligated to reimburse your institution for the expenditure of amounts in excess of the total funds allotted to this grant or cooperative agreement. Your institution is not authorized to continue performance beyond that period covered by the allotted funding and is cautioned to closely manage all available funding, as additional funding will not be provided while the Agency is without appropriations. Any research performed during this time period should be carefully planned, taking into account that NASA technical and administrative personnel will not be available to support these activities during the Government shutdown. Expenses and work should not exceed the funding and time of the award even if additional funding and time is expected. Contact Sponsored Program Services if you have additional questions.
National Endowment for the Humanities (NEH)
NEH is currently shut down. We expect that grant proposals may still be submitted via Grants.gov but per their website, NEH will not update information, process transactions or respond to inquiries until funding is resumed. We also do not expect NEH to issue awards during this period.
Department of Commerce
https://www.commerce.gov/news/blog/2018/12/shutdown-due-lapse-congressional-appropriations
The Department of Commerce includes the following bureaus which are all impacted by the partial shutdown (UConn Storrs and Regional Campuses has funding from agencies that are listed in bold):
Bureau of Economic Analysis (BEA)
Bureau of Industry and Security (BIS)
U.S. Census Bureau
Economic Development Administration (EDA)
Economics and Statistics Administration (ESA)
International Trade Administration (ITA)
Minority Business Development Agency (MBDA)
National Oceanic and Atmospheric Administration (NOAA)
National Telecommunications and Information Administration (NTIA)
National Institute of Standards and Technology (NIST)
U.S. Patent and Trademark Office (USPTO)
The following services and activities will not be available during a lapse except to the extent funded by other than current annual appropriations:
- Most research activities at NIST and NOAA (excluding real-time regular models on research computers used for hurricane and FAA flight planning)
- Assistance and support to recipients of grant funding
- Technical oversight of non-mission essential contracts
- Services and activities provided by:
- Bureau of Economic Analysis (BEA)
- Economic Development Administration (EDA)
- Economics and Statistics Administration (ESA)
- Minority Business Development Agency (MBDA)
- U.S. Census Bureau with the exception of the support of the Decennial Census, which remains funded and activities funded by other agencies and non-Federal entities through reimbursable agreements.
- Most services and activities provided by the International Trade Administration (ITA)
Additionally, electronic systems utilized by the Department of may not be functional (Grants Online which supports EDA and NOAA is not currently functioning).
National Endowment for the Arts (NEA)
NEA is currently shut down. We expect that grant proposals may still be submitted via Grants.gov but per their website, NEH will not post messages or respond. We also do not expect NEH to issue awards during this period.
Department of Transportation
No cooperative agreements, contracts, purchase orders, travel authorizations, or other documents obligating funds will be executed by the Federal Railroad Administration and Federal Transit Administration
USDA – NIFA
NIFA program activities will be suspended during a shutdown. The scope of the activities includes all NIFA extramural funding programs supporting research, education, extension or a combination of two or more of these functions. This includes agency activities associated with competitively awarded, noncompetitive Federal financial assistance payments, capacity and infrastructure, endowment, and all other NIFA grant programs.
Environmental Protection Agency (EPA)
As a general rule, recipients of funded grants and cooperative agreements can continue work on their projects during any EPA shutdown. Grant recipients currently approved to utilize the Automated Standard Application Payment (ASAP) system may make drawdowns of authorized obligated levels during a shutdown. With the exception of grant recipients using ASAP, in the case of government shutdown no payment processing will be available for cost reimbursable or recipients with special award terms and conditions requiring EPA approval prior to payment disbursement (either by paper check, drawdown, or by ACT payment outside to the ASAP system). EPA staff will not be available to make payments until the shutdown ends. Recipients must stop work if they reach a point at which they require EPA involvement or approval.
OVPR Quarterly Reports
Dear Colleagues,
Now that data have been finalized, I would like to provide you with several reports relating to sponsored program activity—both research and education/service—managed by Sponsored Program Services within the Office of the Vice President for Research at UConn and UConn Health. Please visit the OVPR website to view the following reports:
- List of Proposals Submitted: FY18 4th Quarter
- List of Awards Received: FY18 4th Quarter
- Proposals, Awards, Expenditures: FY14-FY18Q4
In the reports, data are presented in two ways: by the PI’s Academic Home Department and by the Managing Department or Center/Institute. Please refer to the first pages of the reports for definitions and information regarding the data. Should you have any questions regarding these quarterly reports, please do not hesitate to contact me.
Please note that we have included an additional Summary of Sponsored Program Activity, which includes the Effective F&A rate on awards. This information provides a snapshot of our activity as compared to the same period last year.
The OVPR continues to seek creative solutions that allow UConn and UConn Health to grow our research enterprise through federal funding, industry partnerships, and collaboration with foundations. I am confident we can continue upward trends by continuing to work together, aggressively applying for extramural funding, and pursuing new channels of support for the tremendous research, scholarship, and creative activities taking place every day at UConn and UConn Health.
Thank you for your continued commitment and contribution to our students, to your research and scholarship, and to UConn/UConn Health.
Sincerely,
Radenka
UConn Health, Jackson Lab To Collaborate On Statewide Pain Consortium
NIH Asks for Your Feedback on a Future Draft Data Management and Sharing Policy
The Office of the Vice President for Research would like to share some information regarding data sharing with researchers who may be affected.
The National Institutes of Health (NIH) issued a Request for Information (RFI) seeking feedback on proposed key provisions to help inform the development of a draft NIH policy for data management and sharing. Submit your comments to NIH by December 10, 2018. Additional information can be found in this NIH blog post, and questions about the proposed provisions may be sent to the NIH Office of Science Policy at SciencePolicy@od.nih.gov
NIH will also be hosting a webinar on the proposed key provisions on November 7, 2018, from 11:30 a.m. – 1:00 p.m. ET.
For questions, please contact Research Compliance Monitor, Ellen Ciesielski at 860.679.6004.
Will NIH require you to register your basic science research in ClinicalTrials.gov?
The Office of the Vice President for Research would like to share some information regarding ClinicalTrials.gov with researchers who may be affected.
NIH has released a Request for Information (RFI), Registration and Results Reporting Standards for Prospective Basic Science Studies Involving Human Participants. This RFI seeks input from the scientific research community and the general public regarding how best to implement the NIH Policy on the Dissemination of NIH-Funded Clinical Trial Information (NOT-OD-16-149) for prospective basic science studies involving human participants. NIH is specifically interested in learning more about studies that meet the NIH definition of a clinical trial (NOT-OD-15-015) but are not defined as applicable clinical trials (42 CFR Part 11), and also meet the definition of fundamental research. You can submit your comments to NIH by November 12, 2018.
For questions about ClinicalTrials.gov, please contact Research Compliance Monitor, Ellen Ciesielski at 860.679.6004.
Are you liable for ClinicalTrials.gov Civil Money Penalties?
The Office of the Vice President for Research would like to share some information regarding ClinicalTrials.gov with researchers who may be affected.
On September 18, 2018, the Food and Drug Administration (FDA) announced a draft guidance titled Civil Money Penalties relating to the Clinical Trials.gov Data Bank. The guidance addresses how the FDA Centers (Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research, and Center for Devices and Radiological Health, for drug, biological, and device products, respectively) identify whether parties have failed to submit required clinical trial registrations, results, or certifications, or knowingly submitted false or misleading information.
The guidance explains that when a responsible party has potentially failed to comply with its disclosure obligations, the FDA will send a Preliminary Notice of Noncompliance Letter, and allow the responsible party 30 days to make corrections. If the FDA determines that the responsible party has still failed to comply, the FDA may issue a Notice of Noncompliance, assess civil monetary penalties, or seek an injunction and/or criminal prosecution. The statutory maximum for civil penalties is “not more than $10,000 for all violations adjudicated in a single proceeding,” plus “not more than $10,000 for each day that the violation continues” past the 30-day notification period.
The deadline to submit your comments to the FDA on this draft is November 20, 2018.
- To check if your trial meets the criteria for ClinicalTrials.gov registration and results posting set forth by the FDA, review this checklist. Applicable clinical trials include those evaluating at least one drug, biological, or device product regulated by the FDA.
- If your NIH-funded study involves human subjects, review this checklist to see if it meets the NIH’s broad definition of a clinical trial and will require registration and results posting. NIH defines a clinical trial as a research study in which one or more human subjects are prospectively assigned to one or more interventions (which may include placebo or other control) to evaluate the effects of those interventions on health-related biomedical or behavioral outcomes.
For questions about ClinicalTrials.gov, please contact Research Compliance Monitor, Ellen Ciesielski at 860.679.6004.
HSPP- July-August-September, 2018- Newsletter
AAHRPP Site Visit 2018
The Association for Accreditation of Human Research Protection Programs (AAHRPP) is an independent, non-profit accrediting body that works to protect the rights and welfare of research participants and promotes high-quality research through an accreditation process.
UConn Health’s Human Subjects Protection Program (HSPP) achieved AAHRPP accreditation in 2006. As an accredited organization, our HSPP must periodically apply for re-accreditation. This is a two-step process. Step 1, which has been completed, consisted of AAHRPP reviewing all of our policies and procedures to ensure they meet regulatory and accreditation standards. Step 2 is an onsite visit by AAHRP representatives to ensure that our policies and procedures are followed. While specific dates have not yet been determined, the next accreditation site visit will occur in the spring of 2019.
During the site visit, representatives from AAHRPP will conduct interviews and review studies records to ensure that policies and procedures have been implemented effectively. AAHRPP representatives will interview the Institutional Official (Wesley Byerly), IRB members, HSPP staff, investigators and research study team members, and individuals that represent various research compliance functions, such as radiation safety, research pharmacy, scientific review, and conflicts of interest. Individuals selected for such interviews will be asked questions about regulatory and ethical issues related to research with human participants and how they interact with the IRB. Investigators and research staff will also be asked about the conduct of their research studies.
In general, topics that may be included during an AAHRPP interview process include:
- Familiarity and compliance with HSPP/IRB polices and procedures
- Roles and responsibilities of investigators and research staff
- Obtaining and documenting informed consent
- Conflict of interest disclosures
- Minimizations of risks to research participants and protecting human subject’s rights and welfare
- Types of training individuals have received in human subject’s protections.
If you are selected for an interview, you will be notified a few weeks prior to the site visit. An educational handout will be provided to help you to prepare.
In addition, you can request an educational session with the Educational Specialist to learn more about the site visit and possible interview questions.
Are you liable for ClinicalTrials.gov Civil Money Penalties?
On September 18, 2018, the Food and Drug Administration (FDA) announced a draft guidance titled Civil Money Penalties relating to the Clinical Trials.gov Data Bank. The guidance addresses how the FDA Centers (Center for Drug Evaluation and Research, Center for Biologics Evaluation and Research, and Center for Devices and Radiological Health, for drug, biological, and device products, respectively) identify whether parties have failed to submit required clinical trial registrations, results, or certifications, or knowingly submitted false or misleading information.
The guidance explains that when a responsible party has potentially failed to comply with its disclosure obligations, the FDA will send a Preliminary Notice of Noncompliance Letter, and allow the responsible party 30 days to make corrections. If the FDA determines that the responsible party has still failed to comply, the FDA may issue a Notice of Noncompliance, assess civil monetary penalties, or seek an injunction and/or criminal prosecution. The statutory maximum for civil penalties is “not more than $10,000 for all violations adjudicated in a single proceeding,” plus “not more than $10,000 for each day that the violation continues” past the 30-day notification period.
The deadline to submit your comments on this draft, electronically or by paper, is November 20, 2018.
- To check if your trial meets the criteria for ClinicalTrials.gov registration and results posting set forth by the FDA, see the checklist found here. Applicable clinical trials include those evaluating at least one drug, biological, or device product regulated by the FDA.
- If your NIH-funded study involves human subjects, check here to see if it meets the NIH’s broad definition of a clinical trial and will require registration and results posting. NIH defines a clinical trial as a research study in which one or more human subjects are prospectively assigned to one or more interventions (which may include placebo or other control) to evaluate the effects of those interventions on health-related biomedical or behavioral outcomes.
- For questions about ClinicalTrials.gov, please contact Research Compliance Monitor, Ellen Ciesielski at 860-679-6004
Does NIH require you to register your basic science research in ClinicalTrials.gov?
NIH has released a Request for Information (RFI), Registration and Results Reporting Standards for Prospective Basic Science Studies Involving Human Participants. This RFI seeks input from the scientific research community and the general public regarding how best to implement the NIH Policy on the Dissemination of NIH-Funded Clinical Trial Information (NOT-OD-16-149) for prospective basic science studies involving human participants. NIH is specifically interested in learning more about studies that meet the NIH definition of a clinical trial (NOT-OD-15-015) but are not defined as applicable clinical trials (42 CFR Part 11), and also meet the definition of fundamental research. You can submit your comments here by November 12, 2018.
Access to Investigational Drugs through Clinical Trials, the Expanded Access Program, or the Right-to-Try Law
An investigational drug is one that has been tested in a laboratory and in animals and is being studied in human for efficacy and safety. Investigational drugs are not yet approved by the Food and Drug Administration (FDA) for use in the general population.
There are various mechanisms through which patients may obtain access to an investigational drug. These mechanisms include 1) clinical trials 2) the FDA’s expanded access program or 3) the recently passed Federal law known as the Right to Try Law. Each of these mechanisms will be discussed below and then compared in table format.
Clinical Trials: The standard mechanism for obtaining access to an investigational drug is through participation in a clinical research trial. A clinical research trial is conducted in accordance with a formal research protocol and its purpose is to evaluate the effectiveness and safety of an investigational drug. To participate in a clinical trial the patient must have the disease or disorder that is being studied and must also meet any specific inclusion or exclusion criteria defined in the research protocol. Patients can search for clinical trials that are being conducted at https://clinicaltrials.gov/.
Expanded Access Program: If participation in a clinical trial is not possible, access to an investigational drug may be sought through the FDA’s Expanded Access Program (EAP).
Access through the EAP may be appropriate when all of the following criteria are met:
- The individual must have a serious/immediately life-threatening disease or terminal condition.
- There must not be a comparable or satisfactory alternative therapy to diagnose, monitor, or treat the disease or condition.
- The individual is unable to participate in a clinical trial.
- Potential patient benefit justifies the potential risks of treatment.
- Providing the drug to the patient will not interfere with the conduct of the clinical trial.
To apply for expanded access, the patient’s physician should first submit a request to the manufacturer of the investigational drug to obtain approval for the use of the product outside of the clinical trial setting. The manufacturer is under no obligation to approve such requests. If the manufacturer will provide the drug, the physician must then submit a request for approval to an Institutional Review Board (IRB) and to the FDA. An IRB is a committee that reviews the plan for the use of the drug to ensure that the rights and welfare of the recipient are protected. If FDA and IRB approval is provided, in the majority of cases the doctor must obtain informed consent from the individual who will receive the drug. The individual’s consent is documented by signing an informed consent form that, among other things, describes the potential risks associated with the drug. More about the FDA’s Expanded Access Program is available at https://www.fda.gov/NewsEvents/PublicHealthFocus/ExpandedAccessCompassionateUse/default.htm
Right to Try Law: The Right-to-Try Law (RTT) was enacted on May 30, 2018. It is intended to provide terminally ill patients a more streamlined mechanism for access to investigational drugs. The Right to Try Law provides a right to request access to the drug. The manufacturer of the drug is under no obligation to grant such requests.
Like the EAP, the RTT law allows for the use of an investigational drug by a patient who has been diagnosed with a life-threatening disease or condition, who has exhausted approved treatment options, and who is unable to participate in a clinical trial involving the eligible investigational drug. An eligible investigational drug means a drug for which a Phase 1 clinical trial has been completed but the drug has still not been fully approved by the FDA. A Phase 1 clinical trial is done primarily to determine the dose of the drug that may be given safely to humans. Determining whether the drug is actually effective comes in later phases of the trial.
Unlike the EAP, the RTT law eliminates the need for approval from the FDA and Institutional Review Board and it provides the sponsor and physician protection from liability associated with harm caused by use of the investigational drug. While the RTT law does specify that the treating physician must obtain the informed consent of the patient, unlike the EAP, the RTT law does not specify the required elements of that informed consent.
Because the RTT law is fairly new, it is not yet clear whether this mechanism will be accepted by manufacturers of investigational drugs.
The following table describes the major similarities and differences of the three current processes by which seriously ill patients may obtain access to investigational drugs.
| Clinical Trials | Expanded Access Program | Right –to Try-Law | |
| Who can participate? | Patients with a condition for which a drug is being developed who meet the inclusion criteria for the trial.
|
Patients with a serious/immediately life-threatening disease or terminal condition, unable to participate in a clinical trial. | Patients with a serious/immediately life-threatening disease or terminal condition, unable to participate in a clinical trial.
|
| Investigational Drug | Not FDA Approved | Not FDA Approved | Not FDA Approved, Phase 1 trial completed
|
| FDA Approval | Required | Required | Not Required |
| IRB Approval | Required | Required | Not Required |
| Informed Consent | Required and must include specific elements required by regulation
|
Required and must include specific elements required by regulation
|
Required, but no specific elements are identified
|
| Manufacturer Obligated to Provide the Investigational Drug | Yes, to those individuals who provide informed consent to participate in the trial | No | No |
| Liability waived for any risk associated with Drug | No | No | Yes |
How can I learn about research studies that are looking for volunteers?
To find ongoing studies that are currently recruiting participants at UConn, you can explore the following online listings:
- Clinical Research Center: https://health.uconn.edu/clinical-research-center/current-research/
- Cancer Trials Office: https://health.uconn.edu/cancer/patient-services/clinical-trials/
- Center on Aging: https://health.uconn.edu/aging/clinical-trials/
- General Listings: https://starr.uchc.edu/Study/BrowseTrials.aspx
- UConn (Kids in Developmental Science) KIDS: https://kids.uconn.edu/join-us/
- Center for Advancement in Managing Pain: https://painresearch.uconn.edu/study/
To search for trials recruiting nationally, please check out the websites below:
- ResearchMatch: https://www.researchmatch.org/about/
- Trials Today: https://www.trialstoday.org/
- ClinicalTrials.gov: https://clinicaltrials.gov/
New OVPR Website
The Office of the Vice President for Research is pleased to present a new and improved website. The new site is still home to all of the important information you need to take care of the day-to-day of your research projects, just in a prettier package. There is some new information as well, including:
- Cross Campus Collaboration resource page
- Training page related to all types of research-related trainings
Please note that the OVPR’s new sites for information pertaining to Storrs, the regional campuses, and UConn Health have new URLs. If you have bookmarked pages, you will need to update to the new URLs.
If you are having trouble locating something you need, please don’t hesitate to contact the relevant service unit. Visit the OVPR Contacts page to find the office or OVPR team you need.
HSPP- April- May-June, 2018 – Newsletter
Clinical Trials – What you need to Know
Did you know the public clinical trials registry, ClinicalTrials.gov, was created in February 2000 in support of a 1997 federal law requiring public registration of clinical trials? It was designed as a web-based catalog of clinical trials to serve as a resource for the patient and research community alike. The law has since expanded to require more types of clinical trials research to be registered, and for some trials, results are also required to be posted.
Did you know there are at least 4 organizations that may require you to register your study on ClinicalTrials.gov? The FDA, National Institutes of Health (NIH), International Committee of Medical Journal Editors (ICMJE) and World Health Organization (WHO) each have rules about registering. For more details on each, please click here.
Did you know the NIH and ICMJE have expanded their definitions of a clinical trial to include behavioral trials? Click here for NIH’s definition. Click here for the ICMJE definition.
Did you know that for studies that require results to be posted per the federal law with completion dates after 1/18/17, a final version of the IRB-approved protocol document and statistical analysis plan must be uploaded to the ClinicalTrials.gov record? Limited information may be redacted. For details, click here.
Should your study be registered with ClinicalTrials.gov?
For more information, see our webpages or contact Ellen Ciesielski (eciesielski@uchc.edu, 860-679-6004) in Research Compliance Services.
Inclusion of Children in Research
When a Principal Investigator (PI) proposes a research project that will involve an intervention or interaction with children, the PI must demonstrate to the IRB that the additional protections afforded to children by regulations have been addressed. The Department of Health and Human Services (DHHS) and the Food and Drug Administration (FDA) have each established regulations governing the inclusion of children in research and the UConn Health IRB has incorporated these regulations into policy. When proposing a research study that will include children as subjects investigators should review the following material:
- IRB Policy 2011-006.0, Additional Protections for Certain Populations – General Policy,
- IRB Policy 2011-006.3, Additional Protections for Certain Populations – Children,
- Form D, Additional Protections for Children Involved as Subjects in Research
In order for the IRB to approve a research protocol that will enroll children, the IRB must assess the information provided by the PI and be able to determine that the research falls within one or more of the following permissible categories and that the plans for obtaining the assent of the child and permission of the parents are appropriate. The examples provided within each category were taken from the Collaborative Institutional Training Initiative (CITI) Program.
Category 1: Research not involving greater than minimal risk.
Minimal risk means that the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests.
To be approvable under this category, the IRB must find that the research presents no greater than “minimal risk” to children, and that adequate provisions are made for soliciting the assent of the children and the permission of their parents or guardians. The IRB may determine that permission from one parent is sufficient.
Examples of Research Projects That May Fall Within Category 1
- A study to determine the relationship between maternal age and head circumference at birth. Measurement of head circumference is part of the normal newborn examination, and is therefore minimal risk.
- A study to determine the incidence of asymptomatic proteinuria in school age children. The research involves the analysis of a voided urine collection, which is minimal risk.
Category 2: Research involving greater than minimal risk but presenting the prospect of direct benefit to the individual subjects.
This category is inclusive of research in which more than minimal risk to children is presented by an intervention or procedure that holds out the prospect of direct benefit for the individual subject, or by a monitoring procedure that is likely to contribute to the subject’s well-being. The IRB may approve research under this category only if the IRB finds and documents that:
(a) The risk is justified by the anticipated benefit to the subjects;
(b) The relation of the anticipated benefit to the risk is at least as favorable to the subjects as that presented by available alternative approaches; and
(c) Adequate provisions are made for soliciting the assent of the children and permission of their parents or guardians. The IRB may determine that permission from one parent is sufficient.
Examples of Research Projects That May Fall Within Category 2:
A pilot study of a shorter duration of antibiotic treatment for uncomplicated otitis media. The potential benefit associated with the shorter duration of treatment is increased compliance, and a reduced rate of antibiotic-related diarrhea. The risk associated with the shorter duration of therapy is a higher likelihood of treatment failure.
The risk associated with this research (e.g. treatment failure) appears to be greater than minimal but can be justified by the anticipated benefit (reduce rate of antibiotic diarrhea); and there is the prospect of direct benefit to the child (increased compliance, shorter exposure time, and a reduced rate of antibiotic-related diarrhea). If the risk-benefit relationship is as favorable as the one seen with standard care (e.g. use of the antibiotic for standard time frame), this research would be approvable under this category.
Use of a placebo, or routine monitoring for safety, is not considered to provide direct benefit to subjects.
Category 3: Research involving greater than minimal risk and no prospect of direct benefit to individual subjects, but likely to yield generalizable knowledge about the subjects’ disorder or condition.
This category is inclusive of research in which more than minimal risk to children is presented by an intervention or procedure that does not hold out the prospect of direct benefit for the individual subject, or by a monitoring procedure which is not likely to contribute to the well-being of the subject. To be approvable under this category, the children to be enrolled must have the disorder or condition under study (i.e. a healthy control group would not be allowable) and the IRB must find and document that:
(a) The risk represents a minor increase over minimal risk;
(b) The intervention or procedure presents experiences to subjects that are reasonably commensurate with those inherent in their actual or expected medical, dental, psychological, social, or educational situations;
(c) The intervention or procedure is likely to yield generalizable knowledge about the subjects’ disorder or condition which is of vital importance for the understanding or amelioration of the subjects’ disorder or condition; and
(d) Adequate provisions are made for soliciting assent of the children and permission of their parents or guardians. In most cases permission from both parents is required.
Examples of Procedures That May Involve Minor Increase Over Minimal Risk:
- Catheterized urine collection
- Skin biopsy or bone marrow biopsy
- MRI scan with sedation
Example of Research That May Fall Within Category 3:
A study to determine the clinical relevance of a new technique to quantitate minimal residual disease (MRD) during therapy for acute lymphoblastic leukemia in children. The study requires one additional bone marrow aspirate be performed during the course of treatment. Therapy for the subject will not be altered based on the results of the assay. However, if it can be shown that the presence of MRD predicts poor outcome, in the future, patients with MRD can receive more intensive treatment and increase their chance of cure.
It can be argued that the risk of a bone marrow aspirate in a child is only a minor increase over minimal risk. Further, the risk appears commensurate with risks inherent in the subject’s actual medical situation, and the research may yield knowledge of vital importance about the child’s disease (leukemia).
Category 4: Research not otherwise approvable which presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health or welfare of children
For research not otherwise approvable that presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health or welfare of children the IRB must find and document:
- That the research presents a reasonable opportunity to further the understanding, prevention, or alleviation of a serious problem affecting the health or welfare of children; and
- b) For studies funded or supported by DHHS, the Secretary, or for studies subject to FDA oversight the Commissioner, after consultation with a panel of experts in pertinent disciplines (for example: science, medicine, education, ethics, law) and following opportunity for public review and comment, has determined either:
(1) that the research in fact satisfies the conditions of one of the aforementioned categories, as applicable, or
(2) (i) the research presents a reasonable opportunity to further the understanding, prevention, or alleviation of a serious problem affecting the health or welfare of children; (ii) the research will be conducted in accordance with sound ethical principles; (iii) adequate provisions are made for soliciting the assent of children and the permission of their parents or guardians.
General Requirements for Assent and Permission:
Assent means an affirmative agreement to participate in research used with those who are not competent or not of legal age to provide informed consent. Failure to object may not be construed as assent.
For children to participate in research, the IRB must determine that adequate provisions are made for soliciting the assent of the children when in the judgment of the IRB the children are capable of providing assent. The IRB will take into account the ages, maturity, and psychological state of the children involved. The judgment may be made for all children to be involved in research under a particular protocol, or for each child. When the IRB determines that assent is required, it shall also determine whether and how assent must be documented.
The IRB may determine that assent is not a necessary condition for proceeding with the research if the capability of some or all of the children is so limited that they cannot reasonably be consulted or that the intervention or procedure involved in the research holds out a prospect of direct benefit that is important to the health or well-being of the children and is available only in the context of the research.
Permission is the agreement of parent(s) or guardian to the participation of their child in research. Permission is generally documented by have the parent(s)/guardian sign an informed consent document.
For research studies not involving greater than minimal risk (Category 1 ) and research involving greater than minimal risk but presenting the prospect of direct benefit to the individual subjects (Category 2) the IRB may find that the permission of one parent or guardian is sufficient. For research studies involving greater than minimal risk and no prospect of direct benefit to individual subjects, but likely to yield generalizable knowledge about the subjects’ disorder or condition (Category 3), and for research studies not otherwise approvable which presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health or welfare of children (Category 4), both parents/guardians must give their permission unless one is deceased, unknown, incompetent or not reasonably available, or unless only one parent has legal responsibility for the care and custody of the child.
If the IRB determines that a research protocol is designed for conditions or for a subject population for which parental or guardian permission is not a reasonable requirement to protect the subject (e.g., neglected or abused children) it may waive the consent requirements provided an appropriate mechanism for protecting the children who will participate as subjects in the research is substituted, and provided further that the waiver is not inconsistent with Federal, state or local law.
The choice of an appropriate mechanism would depend upon the nature and purpose of the activities described in the protocol, the risk and anticipated benefit to the research subjects, and their age, maturity status and condition.
Inclusion or Wards in Research
Children who are wards of the state or any other agency, institution, or entity can be included in research involving greater than minimal risk and no prospect of direct benefit to the individual subjects, but likely to yield generalizable knowledge about the subject’s disorder or condition (Category 3) or research that is not approvable under a defined regulatory category but that presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health or welfare of children (Category 4) only if the research is related to their status as wards, or is conducted in schools, camps, hospitals, organizations, or similar settings in which the majority of children involved as subjects are not wards.
Each child must have an advocate appointed who has the background and experience to act in, and agrees to act in, the best interests of the child, and who is not associated in any way with the research, researchers, or guardian organization.
ResearchMatch training
ResearchMatch.org is a national online recruitment tool, funded by the National Institutes of Health and maintained at Vanderbilt University. ResearchMatch connects researchers with individuals interested in participating in research studies, through its secure, online matching tool. There is no cost to UConn Health researchers to use ResearchMatch.
To learn more about using ResearchMatch for your studies, register for the free ResearchMatch Researcher Webinar Training/Live Demo on Thursday, July 12, 2018 from 3:00 p.m. – 4:00 p.m. The training is open to all research staff. After registering, you will receive a confirmation email with instructions on joining the training.
The team at ResearchMatch will show you how to register your studies, create a cohort of potential volunteers and send out contact messages and surveys. They will also cover how to send a pre-screening (eligibility) survey, contact the volunteers that replied ‘yes’ to your initial message, and manage your enrollment continuum.
To register for the training, click here:
https://attendee.gototraining.com/r/9112903382698216193
For additional information, contact Ellen Ciesielski (eciesielski@uchc.edu; 860-679-6004).
Additional Information on Newly Published Research Policies
The newly published policies for Animal Use in Research, Teaching and Testing and Research Involving Human Subjects revise the existing UConn Storrs policies to establish a uniform regulatory compliance statement that applies to all campuses under which the programs at UConn Health and Storrs operate. A single, overarching policy will help in the development of other policies and procedures to help facilitate cross-campus initiatives.
Key revisions:
- Clarification of who the policies apply to (both policies)
- Revisions to definitions to make them consistent with the regulatory definition (both policies)
- Clarification regarding the role of the Institutional Official and committees (IACUC and IRB)
- Clarification of the authority of the attending veterinarian to be consistent with regulatory requirements (Animal Use policy)
- Clarification of the authority of the IRB to be consistent with regulatory requirements (Human Subjects Research policy)
- Revisions to the enforcement section to make the sections consistent with other university policies (both policies)
- Updated list of authorities (both policies)
The Human Stem Cell Research policy clarifies and updates the existing University-wide policy regarding the type and scope of research to which the policy applies.
The ClinicalTrials.gov policy establishes a new University-wide policy to address FDA, NIH and CMS requirements that applicable trials are registered.
Animal Use in Research, Teaching and Testing: https://policy.uconn.edu/?p=113
Human Stem Cell Research Approval: https://policy.uconn.edu/?p=2453
Human Subjects Research: https://policy.uconn.edu/?p=406
ClinicalTrials.gov: https://policy.uconn.edu/?p=7310
For additional information, contact Ellen Ciesielski (eciesielski@uchc.edu, 860-679-6004)
Revised & New University-Wide Research Policies
The Office of the Vice President for Research (OVPR) Research Compliance Services would like to share some important updates regarding university policies for animal use, human subjects, and stem cell research. These policies were revised to be consistent with federal requirements and are now in effect for all campuses, including UConn Health. A new university-wide policy to address FDA, NIH, and CMS requirements for registration of applicable trials to ClinicalTrials.gov has also been published.
Please see links to published policies below.
ClinicalTrials.gov: https://policy.uconn.edu/?p=7310
Animal Use in Research, Teaching and Testing: https://policy.uconn.edu/?p=113
Human Stem Cell Research Approval: https://policy.uconn.edu/?p=2453
Human Subjects Research: https://policy.uconn.edu/?p=406
For additional information, contact Ellen Ciesielski (eciesielski@uchc.edu, 860-679-6004).
Human Subjects Protection Program – January-February- March , 2018 -Newsletter
Delay of Revised Common Rule and Revised UConn Health IRB Policies
Implementation of the revised version of the Federal regulation governing federally funded/supported research (i.e. 45 CFR 46, also known as the Common Rule) has been delayed until July 19, 2018. In spite of this delay, the UConn Health IRB has moved forward with implementing several changes that aim to reduce regulatory burden on investigators while still offering protection to research participants, complying with current regulatory requirements and being prepared to comply with the revised requirements.
Several IRB forms, templates and policies have been revised. Understanding the reasons for these changes, what has been changed and to what type of research these changes apply may aid investigators in complying with IRB polices as well as with federal regulations.
The following table lists the UConn Health IRB polices that have been changed, a description of the change and the IRB forms that have been modified due to the policy revisions.
| Name of the Revised Policy | Description of the Policy Change | IRB Forms changed due to this Policy Revision |
| 2011-008.0 -Informed Consent – Forms | This policy has been revised to include the additional elements of consent put forth in the revised version of 45 CFR 46.
These elements, while currently optional, will become required for Federal Funded /Supported (FFS) research only if the proposed revised regulation is implemented. If implemented these elements will be required for FFS research initially approved after the effective date of the regulation or for FFS research approved prior to the effective date of the revised rule that is still enrolling subjects and that is being transitioned to review under the revised rule.
While the applicable regulatory criteria for consent will be used as the general premise for all consent forms, when the research is not federally funded or supported, nor subject to FDA oversight, the IRB may exercise judgement when determining if the elements of consent have been appropriately addressed.
New elements of consent:
* The prospective subject or the LAR will be provided with the information that a reasonable person would want to have in order to make an informed decision about whether to participate, and will be given an opportunity to discuss that information. * The ICF must begin with a concise and focused presentation of the key information that is most likely to assist a prospective subject or LAR in understanding the reasons why one might or might not want to participate in the research. This part of the informed consent must be organized and presented in a way that facilitates comprehension.
* Informed consent as a whole presents information in sufficient detail relating to the research, and is be organized and presented in a way that does not merely provide lists of isolated facts, but rather facilitates the prospective subject’s or LAR’s understanding of the reasons why one might or might not want to participate.
*One of the following statements if the research involves the collection of identifiable private information (IPI) or identifiable biospecimens (IB) (i) A statement that identifiers might be removed from the IPI or IB and that, after such removal, the information or biospecimens could be used for future research studies or distributed to another investigator for future research studies without additional informed consent from the subject or the LAR, if this might be a possibility; OR (ii) A statement that the subject’s information or biospecimens collected as part of the research, even if identifiers are removed, will not be used or distributed for future research studies.
* A statement that the subject’s biospecimens (even if identifiers are removed) may be used for commercial profit and whether the subject will or will not share in this commercial profit.
* A statement regarding whether clinically relevant research results, including individual research results, will be disclosed to subjects, and if so, under what conditions.
* For research involving biospecimens, whether the research will (if known) or might include whole genome sequencing (i.e. sequencing of a human germline or somatic specimen with the intent to generate the genome or exome sequence of that specimen). |
|
| Policy 2011-008.1 – Informed Consent – Process | This policy has been changed so that the IRB may approve a non-federally funded or supported research proposal in which an investigator will obtain information or biospecimens for the purpose of screening, recruitment or determining the eligibility of prospective subjects without the informed consent of the prospective subject (and without the need for waivers or alterations), if either of the following conditions is met:
· The investigator will obtain information related to screening, recruiting or determining eligibility through oral or written communication with the prospective subject. · The investigator will obtain identifiable private information or identifiable biospecimens for the purpose of screening, recruiting or determining eligibility by accessing records or stored identifiable biospecimens. * In order to access records or specimens for such purposes, there must be an established relationship between the investigator and the individuals whose records /specimens will be reviewed. * The investigator may delegate the review to designated UConn Health research staff. * Appropriate measures must be in place to protect the confidentiality of the data being utilized.
If the revised regulation is implemented in July this provision will be extended to federally funded/supported research.
Electronic Informed Consent (eIC) Process The investigator should give to the IRB access to the e-consent platform to review the usability of the eIC materials to ensure that they are easy to navigate and that the user may navigate forward or backward within the system, or stop and complete the process at a later time. The investigator must also ensure there is a mechanism in place whereby subjects may ask and obtain answers to questions.
When eIC is proposes subjects must still be provided the option of the consent process occurring in person using a paper based consent form.
|
Text in the IRB application in the section regarding confidentiality has been revised to make it clear that the provisions for protecting the confidentiality of the data as described in the IRB application extend data collected during screening.
|
| Policy 2011-008.2 – Informed Consent – Waivers and Alterations | This policy has been changed to incorporate the new requirement for a waiver or alteration of consent. Per the new requirement, if the research involves using identifiable private information (IPI) or identifiable biospecimens (IB), the investigator must explain why the research could not practicably be carried out without using such IPI or IB. This element is now applicable to all research requesting a waiver or alteration.
This policy also now includes new option to grant a waiver of documentation of consent for non-federally funded or supported research. This new option may apply when the subjects are members of a distinct cultural group or community in which signing forms is not the norm, the research presents no more than minimal risk of harm to subjects and there is an appropriate alternative mechanism for documenting that informed consent was obtained. The IRB will evaluate alternative mechanisms on a case-by-case basis based on information put forth by the PI. If the revised regulation is implemented in July this provision will extend to federally funded / supported non-exempt.
|
Request for Full or Partial Waiver Informed Consent
|
| Policy 2011-008.5 – Informed Consent – Providing and Obtaining Informed Consent
|
This policy has been modified to allow obtaining consent from a “next of kin” for adults who are not mentally retarded.
If the potential participant does not have an appointed legally authorized representative (e.g., individuals designated as having power of attorney for health care, individuals designated as health care representatives) next-of-kin for adults who are not mentally retarded can consent on behalf of a prospective subject as defined in institutional policy 2012-05 titled Legal Representative for Health Care Decisions.
|
None |
| Policy 2011-023.0 – Educational Requirements. | This policy has been changed so that human subjects protection training for all research (exempt, expedited, full board or facilitated review), will be verified for all study personnel at the time of initial approval and on an individual basis at the time a request for modification is received to add a person to the study. In order for training to be considered current it must have been completed within the past three years.
|
none |
| Policy 2011-009.3 –Institutional Review Board – Expedited Reviews | This policy has been changed so that continuing review may not be required for non-federally funded/supported, non-FDA regulated research.
When continuing review is not required, the approval period for an expedited study will be from the date of approval through the expected completion date of the project. If necessary the PI may submit an expedited request for modification to continue the study beyond that date. |
none |
Frequently Asked Questions Related to CITI Training, IRIS System and Facilitated Review
I completed my CITI human subject’s protection training recently. Should I submit my CITI Training Certificate to the IRB?
If an external investigator completed CITI training through another institution, s/he must submit proof of having completed human subject’s protection training to the IRB because the IRB does not get automatically notified of such completions.
If the investigator is affiliated with UConn Health, he/she does not need to submit a certificate of completion. The IRB staff receives the CITI Training certificates one day after individuals have completed the training. Designated IRB staff enter the course completion information into a master training list (Excel) posted in the IRB website and into IRIS. This master training list (Excel) is updated every two weeks. Therefore, investigator should check this list often. In order for the IRB to update the training records in the IRIS system investigators affiliated with UConn Health must have logged into IRIS at least once. Therefore, investigator who have never before log into IRIS should do so right after they have completed the CITI Training. To log into IRIS investigator should click on the following link: https://imedris.uchc.edu , enter their UConn Health network credentials in the ID and PW boxes found in the IRIS logging page, and click on Log in.
I am going to submit an application to UConn Health IRB for review and approval.
Do I need to request an account in IRIS?
Every individual who is affiliated with UConn Health can use the UConn Health ID and password to log into IRIS. Therefore, individuals affiliated with UConn Health (faculty, staff, students, residents, and fellows) do not need to request an account in IRIS.
On the other hand, individuals external to the UConn Health will need to request an account in IRIS. To do so the external investigator must complete the online request form accessible from the IRIS home page. Investigators must complete all the required fields on the form indicating why the account is necessary and with whom at UConn Health he/she will be working. The IRB designated staff may contact the person in UConn Health to confirm that the creation of this account is necessary. Accounts will be created within 1-2 business days.
I have completed an application for IRB review in IRIS. I do not see the sections that allow me to attach documents for review? What should I do?
Unfortunately, the IRIS system currently has a glitch that does not transition the application form to the submission package where you can attach documents. Follow the steps listed below when you get to the last section of the application for initial review and you see a sign stating: “Study Application Completion. You have completed the Study Application process. Click here to go to the …”
- click on the “Back Button” ( located in the upper right hand corner)
- Click on “Study Assistant” menu
- click on “My Studies” sub-menu,
- Open the study, and there you will find Section 1- Submission Packet to the Review Board.
- Click on “Save and Continue to the Next Section” to build the following sections of the forms that will allow you to attach documents.
I am affiliated with UCONN Health (e.g. faculty member, student, employee, or resident, fellow) and I will be part of a study conducted at another institution. That institution has reviewed and approved the study. Do I need approval from the UConn Health IRB?
Yes, if you are affiliated with UConn Health and you are acting in that capacity, your involvement in a research study engages UConn Health in the research and therefore the UConn Health IRB must be involved. However, as opposed to conducting a formal review the UConn Health IRB may elect to rely on the IRB of the other institution. To determine if the UConn Health IRB will do this you, you must submit an application for facilitated review to the UConn Health IRB. By submitting this application you will obtain an official determination from the UConn Health IRB as to whether oversight for the study will be deferred to the external IRB. In order for the UConn Health IRB to defer oversight a written agreement must exist between to the two institutions. This agreement is referred to as an IRB Reliance Agreement. Investigators may contact the IRB to determine if such an agreement is in place or needs to be established.
Annual Individual Financial Disclosure in Research
The Office of the Vice President for Research would like to announce that the 2017 Individual Financial Disclosure in Research reporting period has started today. In order to remain in compliance with university policy and federal regulations, UConn Health employees who are involved in research are required to complete an annual questionnaire in the UConn Health COI-SMART electronic disclosure system.
An automated e-mail inviting applicable employees to complete the questionnaire should be in your inbox. The sender name on the e-mail is UConn Health Financial Disclosure in Research.
If you did not receive an automated e-mail invitation and believe you need to complete the form, or if you have any questions regarding the form or the disclosure requirements, please contact Gus Fernandez-Wolff in the Office of the Vice President for Research, Research Compliance Services at x8125 or gfernandez@uchc.edu.
Thank you for your cooperation.
For more information, contact: Gus Fernandez-Wolff at x8125 or gfernandez@uchc.edu
University Intellectual Property & Commercialization Policy Update
October 22, 2015
Dear Colleagues,
I am pleased to announce that an updated version of the University’s Intellectual Property and Commercialization Policy was approved by the Board of Trustees in early October and is now available online. This comes as the result of a substantive collaboration between the Office of the Vice President for Research, the Provost’s Office, the Office of the General Counsel and faculty and staff at both UConn-Storrs and UConn Health.
Although most of the substantive elements remain the same, the policy now provides a more comprehensive, consistent, and clear explanation of relevant issues, such as the use of University resources by a faculty-affiliated company, conflict of interest disclosures, and the hiring of students to work in faculty-affiliated companies, among others.
We are confident that this streamlined policy document, which applies to faculty, staff, and students at all UConn campuses, more accurately reflects the University’s belief that teaching, research, and economic development are enhanced by the intellectual property generated at UConn.
Should you have any questions related to the updated Intellectual Property and Commercialization Policy, please contact:
| Gregory Gallo, PhD Director Technology Commercialization Services Office of the Vice President for Research Tel. 860-679-3992 gregory.gallo@uconn.edu |
Sincerely,
Dr. Jeff Seemann
Vice President for Research
UConn/UConn Health